
Chinese General Practice ›› 2025, Vol. 28 ›› Issue (06): 655-665.DOI: 10.12114/j.issn.1007-9572.2024.0104
• Frontiers of Medicine • Previous Articles Next Articles
Received:2024-05-10
Revised:2024-09-10
Published:2025-02-20
Online:2024-11-25
Contact:
SUN Kangyun
通讯作者:
孙康云
作者简介:作者贡献:
马弘阳、岳岸娜负责提出研究思路,制订研究目标及文献的搜集、汇总、整理;马弘阳负责撰写文章;岳岸娜负责文章的修订;孙康云负责最终版本修订,对论文整体负责。
基金资助:CLC Number:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2024.0104
| 沉积位置 | 具体表现 |
|---|---|
| 角膜弓 | 弓状脂肪沉积是磷脂和胆固醇沉积在鲍曼膜、角膜基质和后弹力膜的外周角膜中的结果 裂隙灯检查可见外周角膜中有一条宽度为1~1.5 mm的白色环形带与角膜边缘隔离开[ |
| 腱黄色瘤 | 肌腱黄色瘤是结节,常见于跟腱或手、肘部和膝盖皮下可见[ |
| 黄色瘤 | 一种皮肤黄色略微隆起的迹象,通常在眼睑的上部内侧明显[ |
Table 1 Clinical presentation of familial hypercholesterolemia
| 沉积位置 | 具体表现 |
|---|---|
| 角膜弓 | 弓状脂肪沉积是磷脂和胆固醇沉积在鲍曼膜、角膜基质和后弹力膜的外周角膜中的结果 裂隙灯检查可见外周角膜中有一条宽度为1~1.5 mm的白色环形带与角膜边缘隔离开[ |
| 腱黄色瘤 | 肌腱黄色瘤是结节,常见于跟腱或手、肘部和膝盖皮下可见[ |
| 黄色瘤 | 一种皮肤黄色略微隆起的迹象,通常在眼睑的上部内侧明显[ |
| 基因 | 编码蛋白质及其作用 | 染色体位置 | 遗传方式 | 引起的疾病 |
|---|---|---|---|---|
| LDLR | 低密度脂蛋白受体:清除血浆LDL的关键细胞表面受体 | 19p13.1-133 | AD | FH |
| APOB | 载脂蛋白B:LDL颗粒的主要蛋白、LDLR配体 | 2p24.1 | AD | FH |
| PCSK9 | 前蛋白转化酶枯草溶菌素9:在LDLR降解中起作用 | 1p32.3 | AD | FH |
| LDLRAP1 | LDLR衔接蛋白1:与LDLR胞浆相互作用,促进LDL内化 | 1p36.11 | AR | ARH |
| SREBP2 | 胆固醇调节元件结合蛋白-2:主要调控胆固醇生物合成和内稳态相关基因 | 22q13 | AD | FH |
| EPHX2 | 环氧化物水解酶2:具有脂质磷酸酶活性,在血浆脂蛋白颗粒中环氧化物的处理中起作用 | 8p21-p12 | AD | FH |
| CETP | 胆固醇酯转移蛋白,促进胆固醇酯与TG在HDL颗粒和载脂蛋白之间交换 | 16q21 | AD | FH |
| STAP1 | 信号转导适配蛋白家族1:功能未知/不完全与高胆固醇血症相关 | 4q13.2 | AD | FH |
| APOA5 | 载脂蛋白A5:在脂质代谢中发挥重要作用 | 11q23.3 | AD | FH |
| LIPA | 胆固醇酯脂肪酶:水解胆固醇酯或TG | 10q23.31 | AR | 胆固醇酯脂肪酶缺乏症,FH表型 |
| CYP27A1 | 线粒体留醇27-羟化酶,致病性突变可引起脑腱黄色瘤病,这是一种以胆固醇水平轻度开高和黄色瘤为特征的疾病 | 2q33-qter | AR | FH表型 |
| CYP7A1 | 胆固醇7a-羟化酶:致病突变使得体内胆固醇清除障碍 | 8q12.1 | AR | FH表型 |
| PNPLAS | patatin样磷脂酶结构城5:影响脂肪细胞分化、TG水解 | 22q13.31 | AR | FH表型 |
Table 2 Genetic research on FH
| 基因 | 编码蛋白质及其作用 | 染色体位置 | 遗传方式 | 引起的疾病 |
|---|---|---|---|---|
| LDLR | 低密度脂蛋白受体:清除血浆LDL的关键细胞表面受体 | 19p13.1-133 | AD | FH |
| APOB | 载脂蛋白B:LDL颗粒的主要蛋白、LDLR配体 | 2p24.1 | AD | FH |
| PCSK9 | 前蛋白转化酶枯草溶菌素9:在LDLR降解中起作用 | 1p32.3 | AD | FH |
| LDLRAP1 | LDLR衔接蛋白1:与LDLR胞浆相互作用,促进LDL内化 | 1p36.11 | AR | ARH |
| SREBP2 | 胆固醇调节元件结合蛋白-2:主要调控胆固醇生物合成和内稳态相关基因 | 22q13 | AD | FH |
| EPHX2 | 环氧化物水解酶2:具有脂质磷酸酶活性,在血浆脂蛋白颗粒中环氧化物的处理中起作用 | 8p21-p12 | AD | FH |
| CETP | 胆固醇酯转移蛋白,促进胆固醇酯与TG在HDL颗粒和载脂蛋白之间交换 | 16q21 | AD | FH |
| STAP1 | 信号转导适配蛋白家族1:功能未知/不完全与高胆固醇血症相关 | 4q13.2 | AD | FH |
| APOA5 | 载脂蛋白A5:在脂质代谢中发挥重要作用 | 11q23.3 | AD | FH |
| LIPA | 胆固醇酯脂肪酶:水解胆固醇酯或TG | 10q23.31 | AR | 胆固醇酯脂肪酶缺乏症,FH表型 |
| CYP27A1 | 线粒体留醇27-羟化酶,致病性突变可引起脑腱黄色瘤病,这是一种以胆固醇水平轻度开高和黄色瘤为特征的疾病 | 2q33-qter | AR | FH表型 |
| CYP7A1 | 胆固醇7a-羟化酶:致病突变使得体内胆固醇清除障碍 | 8q12.1 | AR | FH表型 |
| PNPLAS | patatin样磷脂酶结构城5:影响脂肪细胞分化、TG水解 | 22q13.31 | AR | FH表型 |
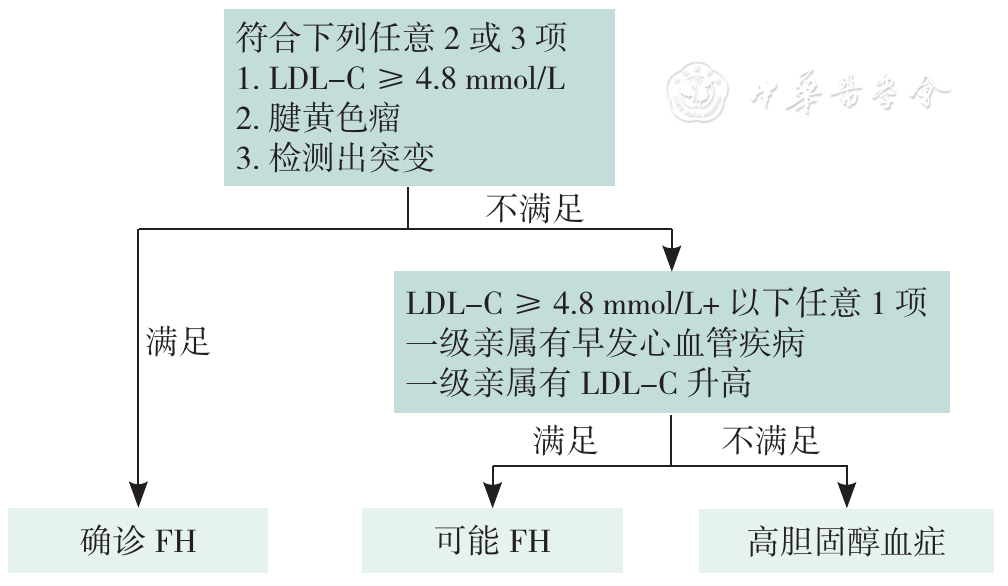
Figure 1 A simplified flow chart of Chinese simplified criteria for familial hypercholesterolemi
| 诊断标准 | 得分(分) |
|---|---|
| 家族史 | |
| 一级亲属已知患有早发冠状动脉和血管疾病,或一级亲属已知LDL-C水平高于第95个百分位数 | 1 |
| 患有腱状黄色瘤和/或角膜弓的一级亲属,或18岁以下且LDL-C水平高于第95个百分位数的儿童 | 2 |
| 临床病史 | |
| 早发的冠状动脉疾病患者 | 2 |
| 早发的脑或周围血管疾病患者 | 1 |
| 身体检查 | |
| 腱黄色瘤 | 6 |
| 45岁之前的角膜弓 | 4 |
| 胆固醇水平 | |
| LDL-C≥330 mg/dL(≥8.5 mmol/L) | 8 |
| LDL-C 250~329 mg/dL(6.5~8.4 mmol/L) | 5 |
| LDL-C 190~249 mg/dL(5.0~6.4 mmol/L) | 3 |
| LDL-C 155~189 mg/dL(4.0~4.9 mmol/L) | 1 |
| 基因分析 | |
| LDLR、APOB或PCSK9的功能突变 | 8 |
| 诊断(诊断基于获得的总分) | |
| 明确的LDL-C | >8 |
| 很可能的LDL-C | 6~8 |
| 可能的LDL-C | 3~5 |
| 不太可能的LDL-C | <3 |
Table 3 Diagnostic criteria of FH proposed by the Dutch Lipid Clinic Network
| 诊断标准 | 得分(分) |
|---|---|
| 家族史 | |
| 一级亲属已知患有早发冠状动脉和血管疾病,或一级亲属已知LDL-C水平高于第95个百分位数 | 1 |
| 患有腱状黄色瘤和/或角膜弓的一级亲属,或18岁以下且LDL-C水平高于第95个百分位数的儿童 | 2 |
| 临床病史 | |
| 早发的冠状动脉疾病患者 | 2 |
| 早发的脑或周围血管疾病患者 | 1 |
| 身体检查 | |
| 腱黄色瘤 | 6 |
| 45岁之前的角膜弓 | 4 |
| 胆固醇水平 | |
| LDL-C≥330 mg/dL(≥8.5 mmol/L) | 8 |
| LDL-C 250~329 mg/dL(6.5~8.4 mmol/L) | 5 |
| LDL-C 190~249 mg/dL(5.0~6.4 mmol/L) | 3 |
| LDL-C 155~189 mg/dL(4.0~4.9 mmol/L) | 1 |
| 基因分析 | |
| LDLR、APOB或PCSK9的功能突变 | 8 |
| 诊断(诊断基于获得的总分) | |
| 明确的LDL-C | >8 |
| 很可能的LDL-C | 6~8 |
| 可能的LDL-C | 3~5 |
| 不太可能的LDL-C | <3 |
| 标准 | 可能性 |
|---|---|
| 成人:TC>7.5 mmol/L(290.0 mg/dL)[或LDL-C>4.9 mmol/L(189.5 mg/dL)] 儿童:TC>6.7 mmol/L(259.1 mg/dL)[或LDL-C>4.0 mmol/L(154.7 mg/dL)] 以及:患者的肌腱黄色瘤或一级/二级亲属 或者:存在LDLR、APOB或PCSK9突变 | 确定 |
| 成人:TC>7.5 mmol/L(290.0 mg/dL)[或LDL-C >4.9 mmol/L(189.5 mg/dL)] 儿童:TC>6.7 mmol/L(259.1 mg/dL)[或LDL-C>4.0 mmol/L(154.7 mg/dL)] 以及:二级亲属心肌梗死家族史<50岁或一级亲属<60岁 或者:一级或二级亲属的TC家族史>7.5 mmol/L(290.0 mg/dL) | 可能 |
Table 4 Diagnostic criteria of FH proposed by the Simon Broome
| 标准 | 可能性 |
|---|---|
| 成人:TC>7.5 mmol/L(290.0 mg/dL)[或LDL-C>4.9 mmol/L(189.5 mg/dL)] 儿童:TC>6.7 mmol/L(259.1 mg/dL)[或LDL-C>4.0 mmol/L(154.7 mg/dL)] 以及:患者的肌腱黄色瘤或一级/二级亲属 或者:存在LDLR、APOB或PCSK9突变 | 确定 |
| 成人:TC>7.5 mmol/L(290.0 mg/dL)[或LDL-C >4.9 mmol/L(189.5 mg/dL)] 儿童:TC>6.7 mmol/L(259.1 mg/dL)[或LDL-C>4.0 mmol/L(154.7 mg/dL)] 以及:二级亲属心肌梗死家族史<50岁或一级亲属<60岁 或者:一级或二级亲属的TC家族史>7.5 mmol/L(290.0 mg/dL) | 可能 |
| 人群 | 标准 |
|---|---|
| 成人 | (1)未经治疗的血清LDL-C>4.7 mmol/L (2)皮肤/腱黄色瘤或脂性角膜弓(<45岁) (3)一级亲属中有FH或早发ASCVD |
| 儿童 | 未治疗的血清LDL-C>3.6 mmol/L且一级亲属中有FH或早发冠心病患者 |
Table 5 2018 Chinese Expert Consensus on Screening and Management of Familial Hypercholesterolemia
| 人群 | 标准 |
|---|---|
| 成人 | (1)未经治疗的血清LDL-C>4.7 mmol/L (2)皮肤/腱黄色瘤或脂性角膜弓(<45岁) (3)一级亲属中有FH或早发ASCVD |
| 儿童 | 未治疗的血清LDL-C>3.6 mmol/L且一级亲属中有FH或早发冠心病患者 |
| 共识标准 | |
|---|---|
| 青少年(年龄<20岁) | 成人(年龄≥20岁) |
| LDL-C≥160 mg/dL(4.1 mmol/L)非HDL≥190 mg/dL(4.9 mmol/L) | LDL-C≥190 md/dL(4.9 mmol/L)非HDL ≥220 mg/dL(5.7 mmol/L) |
| 在下面列出的LDL-C水平下,在一般人群筛查中,FH的概率为80%。以下LDL-C水平应促使临床医生强烈考虑FH的诊断,并获取进一步的家族信息: LDL-C≥250 mg/dL(6.5 mmol/L),年龄≥30岁 LDL-C>220 mg/dL(5.7 mmol/L),年龄20~29岁 LDL-C≥190 mg/dL(4.9 mmol/L),年龄<20岁 | |
Table 6 Expert consensus of management of FH proposed by the National Lipid Association
| 共识标准 | |
|---|---|
| 青少年(年龄<20岁) | 成人(年龄≥20岁) |
| LDL-C≥160 mg/dL(4.1 mmol/L)非HDL≥190 mg/dL(4.9 mmol/L) | LDL-C≥190 md/dL(4.9 mmol/L)非HDL ≥220 mg/dL(5.7 mmol/L) |
| 在下面列出的LDL-C水平下,在一般人群筛查中,FH的概率为80%。以下LDL-C水平应促使临床医生强烈考虑FH的诊断,并获取进一步的家族信息: LDL-C≥250 mg/dL(6.5 mmol/L),年龄≥30岁 LDL-C>220 mg/dL(5.7 mmol/L),年龄20~29岁 LDL-C≥190 mg/dL(4.9 mmol/L),年龄<20岁 | |
| 年龄 | 与FH相关的一级亲属(总胆固醇截断值)(mmol/L) | 与FH相关的二级亲属(总胆固醇截断值)(mmol/L) | 与FH相关的三级亲属(总胆固醇截断值)(mmol/L) | 普通人群(总胆固醇截断值)(mmol/L) |
|---|---|---|---|---|
| <20岁 | 5.7 | 5.9 | 6.2 | 7.0 |
| 20~29岁 | 6.2 | 6.5 | 6.7 | 7.5 |
| 30~39岁 | 7.0 | 7.2 | 7.5 | 8.8 |
| ≥40岁 | 7.5 | 7.8 | 8.0 | 9.3 |
Table 7 Make Early Diagnosis to Prevent Early Death criteria for FH
| 年龄 | 与FH相关的一级亲属(总胆固醇截断值)(mmol/L) | 与FH相关的二级亲属(总胆固醇截断值)(mmol/L) | 与FH相关的三级亲属(总胆固醇截断值)(mmol/L) | 普通人群(总胆固醇截断值)(mmol/L) |
|---|---|---|---|---|
| <20岁 | 5.7 | 5.9 | 6.2 | 7.0 |
| 20~29岁 | 6.2 | 6.5 | 6.7 | 7.5 |
| 30~39岁 | 7.0 | 7.2 | 7.5 | 8.8 |
| ≥40岁 | 7.5 | 7.8 | 8.0 | 9.3 |
| 项目 | 杂合型FH | 纯合型FH | FH家族史 |
|---|---|---|---|
| 临床标准 | 儿童:LDL-C≥160 mg/dL(4.1 mmol/L)成人:LDL-C≥190 mg/dL(4.9 mmol/L)+1个一级亲属,患有类似影响或有早发CAD或阳性基因检测,用于LDL-C升高基因缺陷(LDLR、APOB或PCSK9) | LDL-C≥400 mg/dL(10.3 mmol/L)+父母一方或双方临床诊断为LDL-C、LDL-C升高基因缺陷的阳性基因检测或常染色体隐性遗传性FH或LDL-C>560 mg/dL(14.5 mmol/L)或LDL-C >400 mg/dL(10.3 mmol/L)伴<20岁时患有主动脉瓣疾病或黄色瘤 | LDL-C不作为评判标准;存在已确认FH的一级亲属。 |
| 基因检测 | 存在一个异常的LDL-C升高基因缺陷但LDL-C<160 mg/dL(4.1 mmol/L) 偶尔,杂合子的LDL-C可能>400 mg/dL(10.3 mmol/L),应与纯合子进行类似的治疗 存在异常的LDL-C升高基因缺陷合并降低LDL-C的基因变异使得LDL-C<160 mg/dL(4.1 mmol/L) | 偶尔,纯合子的LDL-C会低于400 mg/dL(10.3 mmol/L) | 未执行基因检测 |
Table 8 A simplified diagnostic criteria for FH proposed by the American Heart Association
| 项目 | 杂合型FH | 纯合型FH | FH家族史 |
|---|---|---|---|
| 临床标准 | 儿童:LDL-C≥160 mg/dL(4.1 mmol/L)成人:LDL-C≥190 mg/dL(4.9 mmol/L)+1个一级亲属,患有类似影响或有早发CAD或阳性基因检测,用于LDL-C升高基因缺陷(LDLR、APOB或PCSK9) | LDL-C≥400 mg/dL(10.3 mmol/L)+父母一方或双方临床诊断为LDL-C、LDL-C升高基因缺陷的阳性基因检测或常染色体隐性遗传性FH或LDL-C>560 mg/dL(14.5 mmol/L)或LDL-C >400 mg/dL(10.3 mmol/L)伴<20岁时患有主动脉瓣疾病或黄色瘤 | LDL-C不作为评判标准;存在已确认FH的一级亲属。 |
| 基因检测 | 存在一个异常的LDL-C升高基因缺陷但LDL-C<160 mg/dL(4.1 mmol/L) 偶尔,杂合子的LDL-C可能>400 mg/dL(10.3 mmol/L),应与纯合子进行类似的治疗 存在异常的LDL-C升高基因缺陷合并降低LDL-C的基因变异使得LDL-C<160 mg/dL(4.1 mmol/L) | 偶尔,纯合子的LDL-C会低于400 mg/dL(10.3 mmol/L) | 未执行基因检测 |
| 类别 | 标准 |
|---|---|
| 临床标准 | |
| LDL-C标准 | 未经治疗的LDL-C>10 mmol/L(>400 mg/dL)提示HoFH,需要进一步检查以确认诊断 |
| 附加标准 | 10岁前皮肤或肌腱黄色瘤和/或未经治疗的LDL-C水平升高,与父母双方的杂合子FH一致 在双基因形式中,父母一方的LDL-C水平可能正常,另一方可能具有与HoFH一致的LDL-C水平 |
| 遗传标准 | LDLR、APOB、PCSK9或LDLRAP1基因不同染色体上双等位基因致病性/可能致病性变异的遗传确认,或不同位点的≥2种此类变异的遗传确认 |
Table 9 The updated diagnostic criteria for HoFH by the European Society of Anaesthesiology
| 类别 | 标准 |
|---|---|
| 临床标准 | |
| LDL-C标准 | 未经治疗的LDL-C>10 mmol/L(>400 mg/dL)提示HoFH,需要进一步检查以确认诊断 |
| 附加标准 | 10岁前皮肤或肌腱黄色瘤和/或未经治疗的LDL-C水平升高,与父母双方的杂合子FH一致 在双基因形式中,父母一方的LDL-C水平可能正常,另一方可能具有与HoFH一致的LDL-C水平 |
| 遗传标准 | LDLR、APOB、PCSK9或LDLRAP1基因不同染色体上双等位基因致病性/可能致病性变异的遗传确认,或不同位点的≥2种此类变异的遗传确认 |
| 标准 | SSCFH | 2018年《家族性高胆固醇血症筛查与诊治中国专家共识》 | DLCN | Simon Broome | NLA专家共识 | MEPED诊断标准 | AHA简化标准 |
|---|---|---|---|---|---|---|---|
| 早发性冠状动脉疾病家族史 | + | + | + | + | + | + | |
| 肌腱黄色瘤家族史 | + | + | |||||
| 高胆固醇血症家族史 | + | + | + | + | + | + | |
| 早发性冠状动脉疾病 | + | + | + | ||||
| 早发性周边血管疾病 | + | ||||||
| 肌腱黄色瘤 | + | + | + | + | + | + | |
| 角膜弓 | + | + | + | ||||
| LDL-C升高 | + | + | + | + | + | + | + |
| 遗传突变 | + | + | + | + | + |
Table 10 Comparison of multiple diagnostic criteria for FH
| 标准 | SSCFH | 2018年《家族性高胆固醇血症筛查与诊治中国专家共识》 | DLCN | Simon Broome | NLA专家共识 | MEPED诊断标准 | AHA简化标准 |
|---|---|---|---|---|---|---|---|
| 早发性冠状动脉疾病家族史 | + | + | + | + | + | + | |
| 肌腱黄色瘤家族史 | + | + | |||||
| 高胆固醇血症家族史 | + | + | + | + | + | + | |
| 早发性冠状动脉疾病 | + | + | + | ||||
| 早发性周边血管疾病 | + | ||||||
| 肌腱黄色瘤 | + | + | + | + | + | + | |
| 角膜弓 | + | + | + | ||||
| LDL-C升高 | + | + | + | + | + | + | + |
| 遗传突变 | + | + | + | + | + |
| 降胆固醇强度 | 药物及其剂量 |
|---|---|
| 高强度(每日剂量可降低LDL-C>50%) | 阿托伐他汀40~80 mg |
| 瑞舒伐他汀20 mg | |
| 中等强度(每日剂量可降低LDL-C 25% ~50%) | 阿托伐他汀10~20 mg |
| 瑞舒伐他汀5~10 mg | |
| 氟伐他汀80 mg | |
| 洛伐他汀40 mg | |
| 匹伐他汀1~4 mg | |
| 普伐他汀40 mg | |
| 辛伐他汀20~40 mg | |
| 血脂康1.2 g |
Table 11 Intensity of statins in lowering cholesterol
| 降胆固醇强度 | 药物及其剂量 |
|---|---|
| 高强度(每日剂量可降低LDL-C>50%) | 阿托伐他汀40~80 mg |
| 瑞舒伐他汀20 mg | |
| 中等强度(每日剂量可降低LDL-C 25% ~50%) | 阿托伐他汀10~20 mg |
| 瑞舒伐他汀5~10 mg | |
| 氟伐他汀80 mg | |
| 洛伐他汀40 mg | |
| 匹伐他汀1~4 mg | |
| 普伐他汀40 mg | |
| 辛伐他汀20~40 mg | |
| 血脂康1.2 g |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [42] |
|
| [43] |
|
| [44] |
|
| [45] |
代海兵,鄢盛恺. 家族性高胆固醇血症的基因诊断研究进展[J]. 临床心血管病杂志,2023,39(5):348-354. DOI:10.13201/j.issn.1001-1439.2023.05.006.
|
| [46] |
|
| [47] |
|
| [48] |
Risk of fatal coronary heart disease in familial hypercholesterolaemia. Scientific steering committee on behalf of the simon broome register group[J]. BMJ,1991,303(6807):893-896. DOI:10.1136/bmj.303.6807.893.
|
| [49] |
中华医学会心血管病学分会动脉粥样硬化及冠心病学组,中华心血管病杂志编辑委员会. 家族性高胆固醇血症筛查与诊治中国专家共识[J]. 中华心血管病杂志,2018,46(2):99-103. DOI:10.3760/cma.j.issn.0253-3758.2018.02.006.
|
| [50] |
|
| [51] |
|
| [52] |
|
| [53] |
中华医学会儿科学分会罕见病学组,中华医学会儿科学分会心血管学组,中华医学会儿科学分会儿童保健学组,等. 儿童脂质异常血症诊治专家共识(2022)[J]. 中华儿科杂志,2022,60(7):633-639.
|
| [54] |
|
| [55] |
|
| [56] |
|
| [57] |
|
| [58] |
|
| [59] |
|
| [60] |
|
| [61] |
|
| [62] |
|
| [63] |
|
| [64] |
蔡雨芯,程仕彤,王绿娅. 2021年《儿童和青少年杂合家族性高胆固醇血症风险评估和临床管理专家共识》解读[J]. 中国实用儿科杂志,2023,38(5):335-340. DOI:10.19538/j.ek2023050603.
|
| [1] | DAI Yao, XUE Liping, ZHANG Shiqi, XU Min, ZHANG Qiu, HU Honglin. Congential Adrenal Hyperplasia Associated with CYP17A1 Gene Mutation: a Case Report and Literature Review [J]. Chinese General Practice, 2025, 28(06): 771-776. |
| [2] | FANG Xiang, SONG Haiqi, LIAO Xiaoyang, LIU Lidi, ZHANG Peng, JIA Yu, YANG Ziyu, YANG Rong, LIU Ruhui. Recommendations for the Management of Hypertensive Disorders of Pregnancy in China: Based on the A Summary of the 2023 Society of Obstetric Medicine of Australia and New Zealand Hypertension in Pregnancy Guideline [J]. Chinese General Practice, 2025, 28(06): 649-654. |
| [3] | NI Xiaojia, LIN Hao, LUO Xufei, KUANG Zhuoran, LIU Yunlan, GUO Jianwen, CHEN Yaolong, CAI Yefeng, Working Group of Clinical Practice Guideline for the Prevention and Treatment of Stroke with Integrated Traditional Chinese and Western Medicine. Clinical Practice Guideline for the Prevention and Treatment of Stroke with Integrated Traditional Chinese and Western Medicine (2023 Edition) [J]. Chinese General Practice, 2025, 28(05): 521-533. |
| [4] | LI Lingqi, GAO Yinyan, ZHANG Yuqin, SUN Dingkui, WU Xinyin, ZHANG Weiru. Survey on the Status and Training Demands of Capabilities for Diagnosing and Treating Common Diseases of Primary Care General Practitioners in Hunan Province [J]. Chinese General Practice, 2025, 28(04): 443-449. |
| [5] | Phillips William R., Sturgiss Elizabeth, Glasziou Paul, olde Hartman Tim C., Orkin Aaron M., Prathivadi Pallavi, Reeve Joanne, Russell Grant M., van Weel Chris. Improving the Reporting of Primary Care Research: Consensus Reporting Items for Studies in Primary Care—the CRISP Statement [J]. Chinese General Practice, 2025, 28(04): 385-392. |
| [6] | GAO Yicheng, YU Zijin, CAO Rui, LIU Zhihan, FANG Rui, LI Yuanyuan, DENG Yingjie, XIANG Wenyuan, FEI Yutong. Thinking and Methodological Suggestions of Empirical Research in the Development of Clinical Practice Guidelines [J]. Chinese General Practice, 2025, 28(04): 402-406. |
| [7] | PENG Hongye, JING Yanan, LIU Dianchun, WANG Ying, XUE Xue, LU Chunli. Domestic and International Advances and Challenges in Early Diagnosis of Prediabetes with Integrated Chinese and Western Medicine [J]. Chinese General Practice, 2025, 28(03): 262-272. |
| [8] | PENG Tao, ZOU Chuan, ZENG Xin, ZHANG Yan, SHEN Jing. A Controlled Study of Salon-training Models Based on the Calgary-Cambridge Guidelines for Improving Patient-physician Communication Skills in General Practice [J]. Chinese General Practice, 2025, 28(01): 71-76. |
| [9] | ZHANG Shuo, ZHANG Long, ZHANG Yan, LI Jianping. Advances in Molecular Biotechnology for Diagnosing and Treating Familial Hypercholesterolemia [J]. Chinese General Practice, 2024, 27(36): 4498-4504. |
| [10] | LI Yuan, MA Hongyang, LI Biao, YUE Anna, SHAO Yaqing, SUN Kangyun. Clinical Significance of Screening for Familial Hypercholesterolemia in Patients with Hypercholesterolemia [J]. Chinese General Practice, 2024, 27(36): 4515-4521. |
| [11] | LU Na, LIU Huaqing, JI Yunxin, GUO Rongjuan, HE Danjun, JIAO Zhian, LIN Yuerui, TIAN Feng, ZHANG Guiqing, XU Zhi, AN Ganghui, ZHANG Yan, YUAN Yonggui. Chinese Expert Consensus on Clinical Diagnosis and Treatment of Test Anxiety Disorder [J]. Chinese General Practice, 2024, 27(34): 4225-4233. |
| [12] | LIU Juan, ZHAO Jing, CHEN Zewen, LI Chang, LI Danling, FU Rong. Application of Head Shaking Tilt Suppression Test and Video Head Impulse Test in the Antidiastole of Vestibular Migraine and Meniere's Disease [J]. Chinese General Practice, 2024, 27(32): 3993-4000. |
| [13] | LYU Guangyu, SUN Wanjun, ZHOU Qianqian, CHEN Xianmeng, LIU Xuehan, HU Xiaowen. Clinical Characteristics and Risk Factors of Patients with Pulmonary Infarction Secondary to Intermediate and High-risk Pulmonary Embolism Misdiagnosed as Pneumonia [J]. Chinese General Practice, 2024, 27(32): 3987-3992. |
| [14] | Diabetes and Microcirculation Professional Committee of Chinese Society of Microcirculation, Primary Endocrine and Metabolic Diseases Group of the Chinese Society of Endocrinology. Expert Consensus on Screening and Prevention of Diabetic Microvascular Disease for Primary Care (2024) [J]. Chinese General Practice, 2024, 27(32): 3969-3986. |
| [15] | QIN Xiaokuan, SUN Kai, FENG Tianxiao, XIAO Xiangyu, WANG Guochen, SU Xiangfei, WEI Xu, ZHU Liguo. Methodological Quality Evaluation and Comprehensive Analysis of Clinical Practice Guidelines and Expert Consensus for Lumbar Disc Herniation [J]. Chinese General Practice, 2024, 27(31): 3857-3864. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||