
Chinese General Practice ›› 2024, Vol. 27 ›› Issue (13): 1608-1615.DOI: 10.12114/j.issn.1007-9572.2023.0334
• Article • Previous Articles Next Articles
Received:2023-06-14
Revised:2023-09-23
Published:2024-05-05
Online:2024-03-06
Contact:
LU Yuan
通讯作者:
陆媛
作者简介:作者贡献:
翟佳燚负责文章构思与设计、资料编码、撰写论文;陆媛负责文章的英文的修订、文章的质量控制及审校,对文章整体负责;刘亚林负责资料编码;陆媛、陶琼英、黄武全、于德华负责论文的修订和监督管理;陶琼英、黄武全负责资源提供。
基金资助:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2023.0334

Figure 1 High frequency word cloud
| 原始语句 | 概念 |
|---|---|
| (1)除了我们家庭医生团队,还有社区居委等部门应该一起参与这项工作。(2)我希望开展这项工作能够明确大家的职责,包括他承担的工作内容等。(3)疾控、社区卫生服务中心、民政部门、地方政府,都应该参加到慢病管理中 | 制定统一标准 |
| (1)现在最关键是你先要让他(患者)知道这个病,如果他什么毛病都不知道,你后面东西没办法弄。(2)我觉得现在公众对MCI认知太薄弱了,早期的(症状)大家很漠视,觉得这就是正常老了,像一个人还能走能跑,就说他MCI,他就觉得像一个玩笑一样 | 对社会公众进行广泛的健康教育 |
| 我可能觉得有的患者比较注重保护隐私,如果他患有MCI,他可能会害怕被别人知道,因为这个东西毕竟现在大家认知不足嘛,担心像老年痴呆一样容易被别人歧视 | 担心因MCI受到歧视 |
| (1)家庭里面子女对老人(患者)的关怀很重要,有些是空巢家庭,(患者)受到的关怀就没那么多。还有子女多的肯定和子女少的是不一样的,但是子女多你没有良心也没用。 (2)家庭如果对他有所关怀的话,我觉得那对他(病情康复)是有促进作用的 | 家人的关怀对患者有利 |
| (1)其实现在医务人员能力不足,(MCI)这个诊断也不是很清楚。 (2)我觉得对认知障碍的这些培训要加强对吧?还有像生活照护的一些技能也需要进行培训 | 工作人员需要进行专业知识技能培训 |
Table 1 Examples of the formation process from the original statement to the initial concept
| 原始语句 | 概念 |
|---|---|
| (1)除了我们家庭医生团队,还有社区居委等部门应该一起参与这项工作。(2)我希望开展这项工作能够明确大家的职责,包括他承担的工作内容等。(3)疾控、社区卫生服务中心、民政部门、地方政府,都应该参加到慢病管理中 | 制定统一标准 |
| (1)现在最关键是你先要让他(患者)知道这个病,如果他什么毛病都不知道,你后面东西没办法弄。(2)我觉得现在公众对MCI认知太薄弱了,早期的(症状)大家很漠视,觉得这就是正常老了,像一个人还能走能跑,就说他MCI,他就觉得像一个玩笑一样 | 对社会公众进行广泛的健康教育 |
| 我可能觉得有的患者比较注重保护隐私,如果他患有MCI,他可能会害怕被别人知道,因为这个东西毕竟现在大家认知不足嘛,担心像老年痴呆一样容易被别人歧视 | 担心因MCI受到歧视 |
| (1)家庭里面子女对老人(患者)的关怀很重要,有些是空巢家庭,(患者)受到的关怀就没那么多。还有子女多的肯定和子女少的是不一样的,但是子女多你没有良心也没用。 (2)家庭如果对他有所关怀的话,我觉得那对他(病情康复)是有促进作用的 | 家人的关怀对患者有利 |
| (1)其实现在医务人员能力不足,(MCI)这个诊断也不是很清楚。 (2)我觉得对认知障碍的这些培训要加强对吧?还有像生活照护的一些技能也需要进行培训 | 工作人员需要进行专业知识技能培训 |
| 编号 | 范畴 | 概念 | 节点(个) |
|---|---|---|---|
| a1 | 制定统一标准 | 政策引导;制定统一标准;明确工作规范 | 15 |
| a2 | 明确职责分工 | 多部门协同,共同发挥作用;明确分工、各司其职 | 19 |
| a3 | 保障合法权益 | 保障医务人员与医疗机构权益;保障患者及其家庭合法权益 | 11 |
| a4 | 监督约束行为 | 对医务人员以及机构依法执业的监督;对媒体宣传监督;对患者行为监督 | 17 |
| a5 | 调配服务资源 | 服务资源丰富程度;资源服务能级 | 9 |
| a6 | 调控服务价格 | 调控医疗服务的价格;调控居家养老服务价格 | 3 |
| a7 | 政策倾斜照顾 | 晋升评优等政策倾斜,提高积极性;对患者有政策关怀,提高服务依从性 | 18 |
| a8 | 引导医患关系 | 政策引导居民与家医签约;引导社会形成良好的医患关系 | 13 |
| a9 | 专项福利津贴 | 对患者提供费用减免;照护支持;福利发放;绿色通道 | 28 |
| a10 | 配置硬件设备 | 医务人员的生产工具;患者自我管理的硬件设施;社会配套设施 | 25 |
| a11 | 加强公众宣教 | 对社会公众进行广泛的健康教育 | 26 |
| a12 | 加大人力投入 | 增加医疗机构岗位设置;组织相关培训;颁发人员资质 | 39 |
| a13 | 普及社会关怀 | 引导全社会对患者进行关怀;不歧视患者并提供帮助 | 16 |
| a14 | 提高创新研发 | 诊疗随访工具研发;生活工具创新研发;"互联网+"技术应用 | 26 |
| a15 | 个人工作动机 | 受个人责任感;工作成就感;工作负荷;自尊心;自我要求 | 18 |
| a16 | 相关工作经验 | 医务人员既往相关工作经验有助于服务的开展 | 4 |
| a17 | 专业知识技能 | 专业知识;技能操作;健康教育技能;心理疏导能力 | 48 |
| a18 | 人文沟通能力 | 服务态度;医患沟通能力;共情能力;爱伤观念;以患者为中心 | 43 |
| a19 | 组织协调能力 | 家庭医生是团队核心;家庭医生需组织调动其他团队角色 | 3 |
| a20 | 慢病管理思维 | 医务人员需具备开展慢病管理的工作思维 | 5 |
| a21 | 团队合作意识 | "医防融合";家医团队应合作完成任务 | 7 |
| a22 | 工作环境创建 | 环境私密性;环境舒适度;环境友善度 | 6 |
| a23 | 工作秩序维护 | 工作秩序有序;医院环境安全 | 4 |
| a24 | 奖惩机制合理 | 多劳多得;突出团队成员价值;制定公平合理奖惩制度;约束团队共同参与 | 17 |
| a25 | 职工能力提升 | 职工继续教育;人文教育;服务技能培训 | 13 |
| a26 | 人员配置合理 | 人员配置合理 | 17 |
| a27 | 任务分配合理 | 任务分配公平合理;整合工作内容、减少重复工作 | 21 |
| a28 | 开展职工关怀 | 医疗机构对职工开展人文关怀;提高组织凝聚力 | 4 |
| a29 | 疾病认知程度 | 患者对疾病的认知 | 31 |
| a30 | 对抗疾病信念 | 患者个人对抗疾病的信念 | 19 |
| a31 | 信息理解能力 | 患者个人信息理解和接受能力 | 24 |
| a32 | 心理因素影响 | 患者对医生不信任;否认、回避、冷漠等心理因素;固执、消极等性格因素 | 14 |
| a33 | 个人道德素养 | 个人道德因素对医患关系的影响 | 4 |
| a34 | 担心因病受歧 | 患者害怕隐私暴露;担心因MCI受到歧视 | 5 |
| a35 | 家庭规模情况 | 家庭人口数量;独居情况 | 19 |
| a36 | 家庭关怀程度 | 家人对患者的关怀程度;家人对患者的疾病康复支持程度 | 26 |
| a37 | 家庭经济水平 | 经济水平影响健康水平;经济水平影响疾病康复 | 22 |
| a38 | 照护体力负担 | 照护者体力负担对照护质量的影响;照护者体力负担对疾病康复的影响 | 17 |
| a39 | 家属心理负担 | 家属心理负担对家庭关系的影响;家属心理负担对患者身心及照护影响 | 5 |
| a40 | 随访连续可及 | 患者信息收集的可及性;随访的连续性影响服务质量效果 | 12 |
| a41 | 服务内容适宜 | 对医务人员积极性的影响;对患者依从性的影响 | 18 |
| a42 | 服务频率合理 | 对医务人员积极性的影响;对患者依从性的影响;对服务效果的影响 | 16 |
| a43 | 生产工具实用 | 采用实用、简便的工具;整合并改进各类信息平台 | 7 |
| a44 | 工作方法高效 | 工作方法对依从性、服务效果、效率的影响 | 23 |
| a45 | 服务效果正向 | 患者的满意度;慢病管理服务干预的效果 | 17 |
| a46 | 社会效益产出 | 减少疾病的发生发展;减轻疾病负担 | 12 |
| a47 | 适宜模式便捷 | 具有可行性;可操作性强 | 19 |
| a48 | 成本消耗合理 | 时间成本;人力成本;资金成本 | 11 |
| a49 | 考核评估合理 | 立足于疾病特点;合理的考核方案;质量评估指标适宜 | 16 |
Table 2 Concepts and categories formed by open coding
| 编号 | 范畴 | 概念 | 节点(个) |
|---|---|---|---|
| a1 | 制定统一标准 | 政策引导;制定统一标准;明确工作规范 | 15 |
| a2 | 明确职责分工 | 多部门协同,共同发挥作用;明确分工、各司其职 | 19 |
| a3 | 保障合法权益 | 保障医务人员与医疗机构权益;保障患者及其家庭合法权益 | 11 |
| a4 | 监督约束行为 | 对医务人员以及机构依法执业的监督;对媒体宣传监督;对患者行为监督 | 17 |
| a5 | 调配服务资源 | 服务资源丰富程度;资源服务能级 | 9 |
| a6 | 调控服务价格 | 调控医疗服务的价格;调控居家养老服务价格 | 3 |
| a7 | 政策倾斜照顾 | 晋升评优等政策倾斜,提高积极性;对患者有政策关怀,提高服务依从性 | 18 |
| a8 | 引导医患关系 | 政策引导居民与家医签约;引导社会形成良好的医患关系 | 13 |
| a9 | 专项福利津贴 | 对患者提供费用减免;照护支持;福利发放;绿色通道 | 28 |
| a10 | 配置硬件设备 | 医务人员的生产工具;患者自我管理的硬件设施;社会配套设施 | 25 |
| a11 | 加强公众宣教 | 对社会公众进行广泛的健康教育 | 26 |
| a12 | 加大人力投入 | 增加医疗机构岗位设置;组织相关培训;颁发人员资质 | 39 |
| a13 | 普及社会关怀 | 引导全社会对患者进行关怀;不歧视患者并提供帮助 | 16 |
| a14 | 提高创新研发 | 诊疗随访工具研发;生活工具创新研发;"互联网+"技术应用 | 26 |
| a15 | 个人工作动机 | 受个人责任感;工作成就感;工作负荷;自尊心;自我要求 | 18 |
| a16 | 相关工作经验 | 医务人员既往相关工作经验有助于服务的开展 | 4 |
| a17 | 专业知识技能 | 专业知识;技能操作;健康教育技能;心理疏导能力 | 48 |
| a18 | 人文沟通能力 | 服务态度;医患沟通能力;共情能力;爱伤观念;以患者为中心 | 43 |
| a19 | 组织协调能力 | 家庭医生是团队核心;家庭医生需组织调动其他团队角色 | 3 |
| a20 | 慢病管理思维 | 医务人员需具备开展慢病管理的工作思维 | 5 |
| a21 | 团队合作意识 | "医防融合";家医团队应合作完成任务 | 7 |
| a22 | 工作环境创建 | 环境私密性;环境舒适度;环境友善度 | 6 |
| a23 | 工作秩序维护 | 工作秩序有序;医院环境安全 | 4 |
| a24 | 奖惩机制合理 | 多劳多得;突出团队成员价值;制定公平合理奖惩制度;约束团队共同参与 | 17 |
| a25 | 职工能力提升 | 职工继续教育;人文教育;服务技能培训 | 13 |
| a26 | 人员配置合理 | 人员配置合理 | 17 |
| a27 | 任务分配合理 | 任务分配公平合理;整合工作内容、减少重复工作 | 21 |
| a28 | 开展职工关怀 | 医疗机构对职工开展人文关怀;提高组织凝聚力 | 4 |
| a29 | 疾病认知程度 | 患者对疾病的认知 | 31 |
| a30 | 对抗疾病信念 | 患者个人对抗疾病的信念 | 19 |
| a31 | 信息理解能力 | 患者个人信息理解和接受能力 | 24 |
| a32 | 心理因素影响 | 患者对医生不信任;否认、回避、冷漠等心理因素;固执、消极等性格因素 | 14 |
| a33 | 个人道德素养 | 个人道德因素对医患关系的影响 | 4 |
| a34 | 担心因病受歧 | 患者害怕隐私暴露;担心因MCI受到歧视 | 5 |
| a35 | 家庭规模情况 | 家庭人口数量;独居情况 | 19 |
| a36 | 家庭关怀程度 | 家人对患者的关怀程度;家人对患者的疾病康复支持程度 | 26 |
| a37 | 家庭经济水平 | 经济水平影响健康水平;经济水平影响疾病康复 | 22 |
| a38 | 照护体力负担 | 照护者体力负担对照护质量的影响;照护者体力负担对疾病康复的影响 | 17 |
| a39 | 家属心理负担 | 家属心理负担对家庭关系的影响;家属心理负担对患者身心及照护影响 | 5 |
| a40 | 随访连续可及 | 患者信息收集的可及性;随访的连续性影响服务质量效果 | 12 |
| a41 | 服务内容适宜 | 对医务人员积极性的影响;对患者依从性的影响 | 18 |
| a42 | 服务频率合理 | 对医务人员积极性的影响;对患者依从性的影响;对服务效果的影响 | 16 |
| a43 | 生产工具实用 | 采用实用、简便的工具;整合并改进各类信息平台 | 7 |
| a44 | 工作方法高效 | 工作方法对依从性、服务效果、效率的影响 | 23 |
| a45 | 服务效果正向 | 患者的满意度;慢病管理服务干预的效果 | 17 |
| a46 | 社会效益产出 | 减少疾病的发生发展;减轻疾病负担 | 12 |
| a47 | 适宜模式便捷 | 具有可行性;可操作性强 | 19 |
| a48 | 成本消耗合理 | 时间成本;人力成本;资金成本 | 11 |
| a49 | 考核评估合理 | 立足于疾病特点;合理的考核方案;质量评估指标适宜 | 16 |
| 编号 | 主范畴 | 范畴 | 节点(个) | 频率(%) |
|---|---|---|---|---|
| A1 | 政策导向作用 | a1制定统一标准,a2明确职责分工,a3保障合法权益,a4监督约束行为, a5调配服务资源,a6调控服务价格,a7政策倾斜照顾,a8引导医患关系 | 105 | 12.93 |
| A2 | 政府投入支持 | a9专项福利津贴,a10配置硬件设备,a11加强公众宣教, a12加大人力投入,a13普及社会关怀,a14提高创新研发 | 160 | 19.70 |
| A3 | 工作人员效能 | a15个人工作动机,a16相关工作经验,a17专业知识技能, a18人文沟通能力,a19组织协调能力,a20慢病管理思维,a21团队合作意识 | 128 | 15.76 |
| A4 | 医疗机构管理 | a22工作环境创建,a23工作秩序维护,a24奖惩机制合理, a25职工能力提升,a26人员配置合理,a27任务分配合理,a28开展职工关怀 | 82 | 10.10 |
| A5 | 患者配合程度 | a29疾病认知程度,a30对抗疾病信念,a31信息理解能力, a32心理因素影响,a33个人道德素养,a34担心因病受歧 | 97 | 11.95 |
| A6 | 患者家庭支持 | a35家庭规模情况,a36家庭关怀程度,a37家庭经济水平,a38照护体力负担,a39家属心理负担 | 89 | 10.96 |
| A7 | 任务执行过程 | a40随访连续可及,a41服务内容适宜,a42服务频率合理,a43生产工具实用,a44工作方法高效 | 76 | 9.36 |
| A8 | 任务执行结果 | a45服务效果正向,a46社会效益产出,a47模式整体便捷,a48成本消耗合理,a49考核评估合理 | 75 | 9.24 |
Table 3 Main categories formed by principal axis coding
| 编号 | 主范畴 | 范畴 | 节点(个) | 频率(%) |
|---|---|---|---|---|
| A1 | 政策导向作用 | a1制定统一标准,a2明确职责分工,a3保障合法权益,a4监督约束行为, a5调配服务资源,a6调控服务价格,a7政策倾斜照顾,a8引导医患关系 | 105 | 12.93 |
| A2 | 政府投入支持 | a9专项福利津贴,a10配置硬件设备,a11加强公众宣教, a12加大人力投入,a13普及社会关怀,a14提高创新研发 | 160 | 19.70 |
| A3 | 工作人员效能 | a15个人工作动机,a16相关工作经验,a17专业知识技能, a18人文沟通能力,a19组织协调能力,a20慢病管理思维,a21团队合作意识 | 128 | 15.76 |
| A4 | 医疗机构管理 | a22工作环境创建,a23工作秩序维护,a24奖惩机制合理, a25职工能力提升,a26人员配置合理,a27任务分配合理,a28开展职工关怀 | 82 | 10.10 |
| A5 | 患者配合程度 | a29疾病认知程度,a30对抗疾病信念,a31信息理解能力, a32心理因素影响,a33个人道德素养,a34担心因病受歧 | 97 | 11.95 |
| A6 | 患者家庭支持 | a35家庭规模情况,a36家庭关怀程度,a37家庭经济水平,a38照护体力负担,a39家属心理负担 | 89 | 10.96 |
| A7 | 任务执行过程 | a40随访连续可及,a41服务内容适宜,a42服务频率合理,a43生产工具实用,a44工作方法高效 | 76 | 9.36 |
| A8 | 任务执行结果 | a45服务效果正向,a46社会效益产出,a47模式整体便捷,a48成本消耗合理,a49考核评估合理 | 75 | 9.24 |
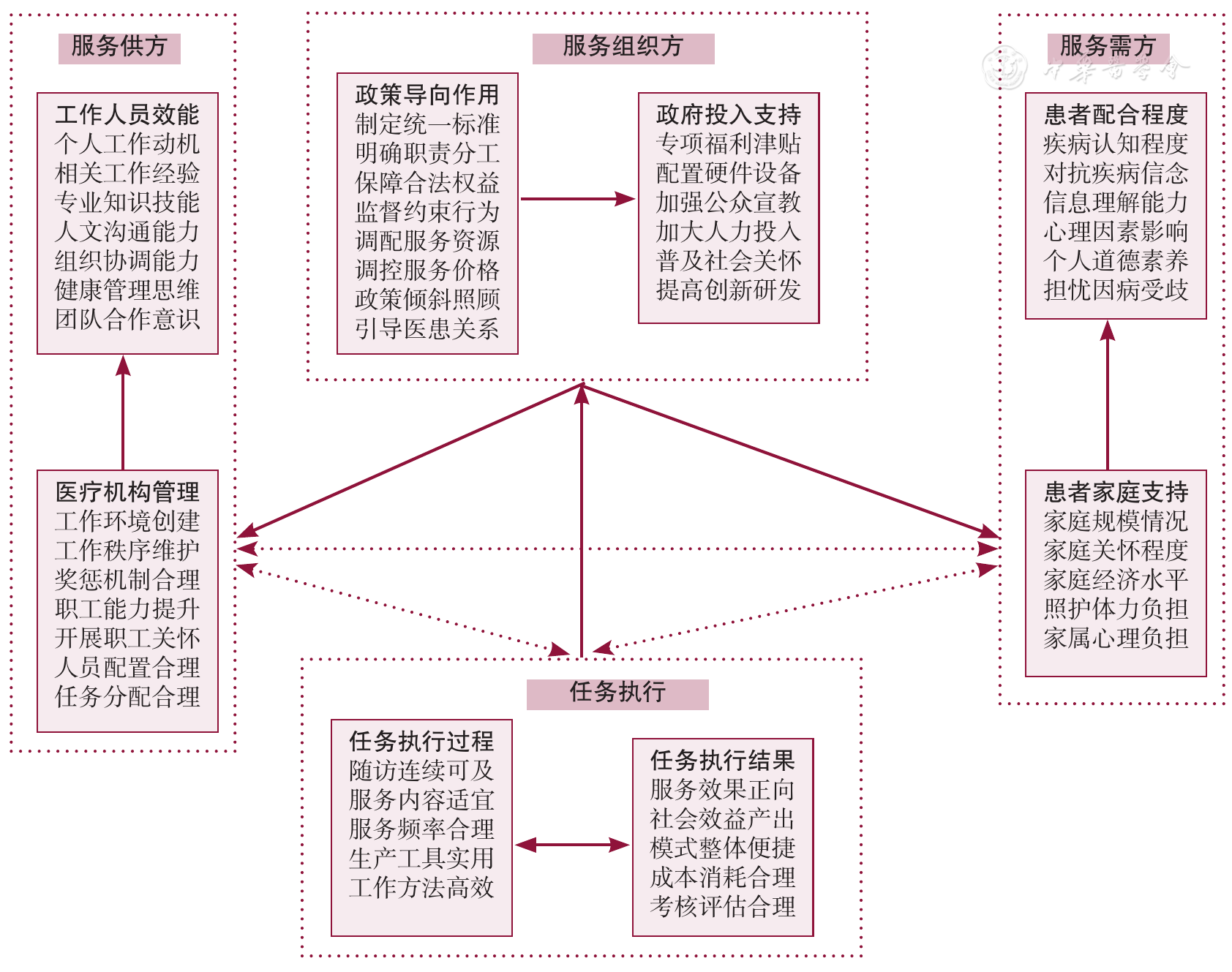
Figure 2 The theoretical framework of factors influencing the performance of service model of family doctor teams for the MCI population
| [1] |
Risk Reduction of Cognitive Decline and Dementia:WHO Guidelines[M]. Geneva:World Health Organization,2019.
|
| [2] |
|
| [3] |
|
| [4] |
刘亚林,陆媛,徐圣明,等. 全科医生认知功能评估量表在轻度认知功能障碍筛查中的应用研究[J]. 中国全科医学,2021,24(22):2819-2825. DOI:10.12114/j.issn.1007-9572.2021.00.228.
|
| [5] |
陈佳,叶子容,袁满琼,等. 蒙特利尔认知评估量表在轻度认知功能障碍筛查中的应用与进展[J]. 中华精神科杂志,2017,50(5):386-389. DOI:10.3760/cma.j.issn.1006-7884.2017.05.014.
|
| [6] |
杨丽,严静,金煜,等. 浙江省养老院老年人痴呆和轻度认知障碍患病率及其相关因素分析[J]. 中华老年医学杂志,2020,39(12):1462-1467. DOI:10.3760/cma.j.issn.0254-9026.2020.12.022.
|
| [7] |
中国痴呆与认知障碍诊治指南写作组,中国医师协会神经内科医师分会认知障碍疾病专业委员会. 2018中国痴呆与认知障碍诊治指南(五):轻度认知障碍的诊断与治疗[J]. 中华医学杂志,2018,98(17):1294-1301. DOI:10.3760/cma.j.issn.0376-2491.2018.17.003.
|
| [8] |
中国健康管理协会. 慢性病健康管理规范(T/CHAA 007-2019)[J]. 中华预防医学杂志,2020,54(1):39-41. DOI:10.3760/cma.j.issn.0253-9624.2020.01.009.
|
| [9] | |
| [10] |
何昊,关青,张浩波,等. 新版轻度认知障碍临床指南概要[J]. 中华诊断学电子杂志,2018,6(3):145-150. DOI:10.3877/cma.j.issn.2095-655X.2018.03.001.
|
| [11] | |
| [12] |
王晶,何昊,邱月虹,等. 轻度认知障碍的认知干预研究进展[J]. 中华行为医学与脑科学杂志,2019,28(1):85-90. DOI:10.3760/cma.j.issn.1674-6554.2019.01.016.
|
| [13] |
赵霞,葛晨希,王丽娜,等. 轻度认知障碍认知训练技术及策略[J]. 中华行为医学与脑科学杂志,2019,28(3):212-217. DOI:10.3760/cma.j.issn.1674-6554.2019.03.004.
|
| [14] |
方红,盛建华,邱朝晖. 家庭医生制服务模式对老年轻度认知功能障碍干预效果的研究[J]. 老年医学与保健,2015,21(2):115-118. DOI:10.3969/j.issn.1008-8296.2015-16.
|
| [15] |
杜学鹏,零春晴,吴爽,等. 我国家庭医生激励机制研究——基于波特—劳勒综合型激励模型[J]. 卫生经济研究,2019,36(3):22-25. DOI:10.14055/j.cnki.33-1056/f.2019.03.007.
|
| [16] |
卢慧敏,黄琦,杨丹丹,等. 家庭医生团队职业倦怠现状及影响因素研究[J]. 中国全科医学,2019,22(10):1223-1228. DOI:10.12114/j.issn.1007-9572.2019.10.018.
|
| [17] |
黄翠玲,寿涓,李娅玲,等. 上海市"1+1+1"医疗机构组合签约策略实施现状的质性研究[J]. 中国全科医学,2019,22(19):2308-2313. DOI:10.12114/j.issn.1007-9572.2019.00.074.
|
| [18] |
谢文野. "医养结合"养老的家庭医生服务模式的伦理优势、问题分析与对策[J]. 中国医学伦理学,2018,31(4):519-524. DOI:10.12026/j.issn.1001-8565.2018.04.24.
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
陈宝欣,忽群,孙明伟,等. 家庭医生团队"三师共管"社区老年慢性病健康管理模式构建与效果评价[J]. 中国医学创新,2020,17(15):164-168. DOI:10.3969/j.issn.1674-4985.2020.15.042.
|
| [27] | |
| [28] |
范明林,吴军,马丹丹. 质性研究方法[M]. 2版. 上海:格致出版社,2018.
|
| [29] |
陈向明. 质的研究方法与社会科学研究[M]. 北京:教育科学出版社,2000.
|
| [30] |
李燕萍,熊向清. 保险企业核心员工忠诚度的影响因素及与绩效的关系研究——基于抽样调查的实证分析[J]. 保险研究,2017(9):86-100. DOI:10.13497/j.cnki.is.2017.09.008.
|
| [31] |
赵红霞,袁媛,郑鑫. 基于知信行理论的延续性护理对冠心病患者服药依从性、生活质量及自我效能的影响[J]. 中华健康管理学杂志,2020,6(4):356-361.
|
| [32] |
汪文新,江舜杰,陈美林,等. 基于CiteSpace近15年来我国医患关系领域研究热点探讨[J]. 中国卫生事业管理,2018,35(5):340-342.
|
| [1] | LIU Xin, WEI Yanan, LIU Jie, WANG Jingtong. Research of Influencing Factors for Physical Impairment Combined with Cognitive Impairment in the Elderly [J]. Chinese General Practice, 2024, 27(26): 3281-3288. |
| [2] | WANG Chenyu, ZHANG Chen, SHI Lulu, ZHU Mengna, WANG Lina. Advances in Cognitive Function Health Management Strategies for Individuals with Mild Cognitive Impairment in Community [J]. Chinese General Practice, 2024, 27(26): 3273-3280. |
| [3] | FENG Zihang, ZHU Yaning, SUN Ying, LUO Ruzhen, CHEN Hongbo, LIU Jingying, CHENG Ranran, LIU Yanhui. Latent Class Analysis and Influence Factors Study of Cognitive Function among Older People with Chronic Diseases in Community [J]. Chinese General Practice, 2024, 27(26): 3289-3296. |
| [4] | FENG Yuhui, LI Shanshan, TAO Jianwen, HUANG Yanyan. Cognitive Impairment in the Elderly: a Survey and Analysis of Influencing Factors [J]. Chinese General Practice, 2024, 27(26): 3297-3303. |
| [5] | ZHAO Ting, ZHANG Yan, WU Lanxin, MENG Lixue, LIU Li. A Qualitative Study of Community-dwelling Elderly People' Experience of Multimorbidity [J]. Chinese General Practice, 2024, 27(25): 3143-3149. |
| [6] | LI Lisha, TANG Qi, WANG Cao, WU Wenhui, WU Huanyun, GAO Zhenqi, CAO Wenfang, LYU Jun. The Influence of Rational Drug Use Management Mode of the Elderly in Community on Patients' Knowledge, Attitude and Practice of Drug Use [J]. Chinese General Practice, 2024, 27(25): 3129-3135. |
| [7] | LI Xiaochun, HAO Mo, LI Chengyue, PU Chuan. Appropriateness of Resource Allocation of Chronic Diseases Prevention and Control in Chongqing [J]. Chinese General Practice, 2024, 27(25): 3178-3183. |
| [8] | LIANG Wannian, LIU Jue. Construct the China Academic Community of General Practitioners/Family Physicians to Promote the High-quality Development of the General Practice Discipline [J]. Chinese General Practice, 2024, 27(25): 0-D. |
| [9] | WANG Lin, WANG Yixin, CHEN Tingyan, LIN Shaohai, ZHANG Yonghui. Discussion on the Practice of Narrative Medicine in Primary Care from the Perspective of General Practitioners [J]. Chinese General Practice, 2024, 27(24): 3057-3060. |
| [10] | HU Guiping, LIN Ping, ZHAO Zhenjuan, WANG Yini, YAN Mingqiang, SUN Xiao. Relationship between Dietary Inflammatory Potential and Severity of Coronary Artery Disease in Acute Coronary Syndrome Patients [J]. Chinese General Practice, 2024, 27(24): 3000-3006. |
| [11] | LIU Xiaogang, YANG Shicheng, FU Naikuan, SHAO Dujing, ZHANG Peng. The Impact of Dapagliflozin on the Incidence of Contrast-induced Nephropathy in Patients with Type 2 Diabetes Mellitus Underwent Percutaneous Coronary Intervention [J]. Chinese General Practice, 2024, 27(24): 2994-2999. |
| [12] | TU Shuting, LIN Jiaying, ZHUANG Jinyang, XIANG Jingnan, WEI Dongshuai, XIE Yong, JIA Jie. Incidence and Related Factors of Post-stroke Cognitive Impairment: a Multicenter Cross-sectional Study Based on Full-cycle Rehabilitation in Stroke [J]. Chinese General Practice, 2024, 27(23): 2829-2837. |
| [13] | LI Mingzhe, TIAN Yichuan, WANG Chenglong, WANG Jingjing. Study on the Independent and Joint Effects of Physical Activity and Sleep on Low Back Pain in Middle-aged and Elderly Adults [J]. Chinese General Practice, 2024, 27(23): 2869-2874. |
| [14] | XU Zhijie, WANG Yang, QIAN Yi. The Design and Application of In-depth Interview in Primary Care Research [J]. Chinese General Practice, 2024, 27(22): 2797-2806. |
| [15] | YANG Sen, ZHAO Huaxin, GE Xuhua, MA Le, JIN Hua, XIE Mujin, PU Zhen, BAI Zhaohui, YU Dehua. Impact of an Integrated Hospital-community-patient Chronic Disease Management Pathway on Postoperative Colorectal Cancer Patients [J]. Chinese General Practice, 2024, 27(22): 2724-2730. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||