
Chinese General Practice ›› 2024, Vol. 27 ›› Issue (01): 15-26.DOI: 10.12114/j.issn.1007-9572.2022.0852
Special Issue: 指南/共识最新文章合集; 心理健康最新文章合集
• Research on General Practice Work • Previous Articles Next Articles
Received:2023-04-26
Revised:2023-07-25
Published:2024-01-05
Online:2023-10-23
Contact:
Searle Kendall
通讯作者:
Searle Kendall
作者简介:
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.chinagp.net/EN/10.12114/j.issn.1007-9572.2022.0852
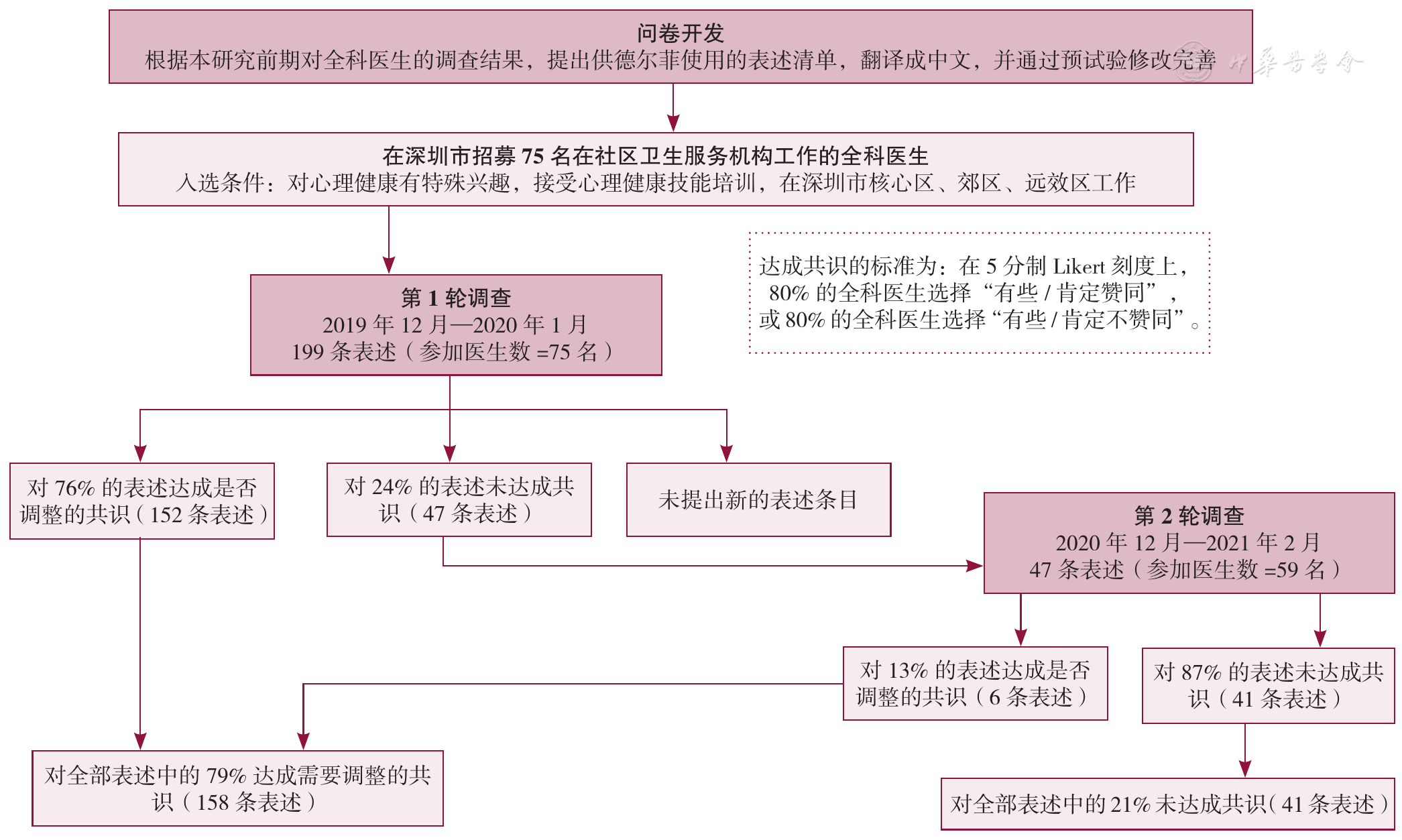
Figure 1 Delphi process from questionnaire development to statement consensus
| mhGAP-IG.v2中涉及抑郁的主题 | 第1轮(n=75) | 第2轮(n=59) | 总体共识 | |||||
|---|---|---|---|---|---|---|---|---|
| 表述条目数(条) | 达成调整共识的条目(%) | 平均分(分) | 表述条目数(条) | 达成调整共识的条目(%) | 平均分(分) | 达成调整共识的条目(%) | 平均分(分) | |
| "以人为本"的指南 | 18 | 100 | 4.65 | 0 | 0 | 0 | 100 | 4.65 |
| 抑郁障碍的表现特征 | 28 | 64 | 4.07 | 10 | 0 | 3.50 | 64 | 4.06 |
| 筛查工具的获得和使用 | 11 | 64 | 4.13 | 4 | 25 | 3.80 | 73 | 4.24 |
| 医疗服务及社区系统的内部关系 | 28 | 79 | 4.23 | 6 | 17 | 3.75 | 82 | 4.26 |
| 药物治疗选择 | 18 | 78 | 4.20 | 4 | 0 | 3.51 | 78 | 4.19 |
| 双相障碍中的躁狂和抑郁发作 | 4 | 100 | 4.59 | 0 | 0 | 0 | 100 | 4.59 |
| 与患者和社区针对抑郁进行沟通 | 29 | 90 | 4.36 | 3 | 0 | 3.77 | 90 | 4.36 |
| 随访 | 33 | 61 | 4.03 | 13 | 31 | 3.64 | 73 | 4.05 |
| 管理患者信息 | 11 | 82 | 4.20 | 2 | 0 | 3.73 | 82 | 4.20 |
| 指南的整体结构 | 19 | 74 | 4.06 | 5 | 0 | 3.61 | 74 | 4.06 |
| 总体共识 | 199 | 76 | 4.25 | 47 | 13 | 3.66 | 79 | 4.26 |
Table 1 Wave 1 & 2 Delphi survey consensus by thematic domains
| mhGAP-IG.v2中涉及抑郁的主题 | 第1轮(n=75) | 第2轮(n=59) | 总体共识 | |||||
|---|---|---|---|---|---|---|---|---|
| 表述条目数(条) | 达成调整共识的条目(%) | 平均分(分) | 表述条目数(条) | 达成调整共识的条目(%) | 平均分(分) | 达成调整共识的条目(%) | 平均分(分) | |
| "以人为本"的指南 | 18 | 100 | 4.65 | 0 | 0 | 0 | 100 | 4.65 |
| 抑郁障碍的表现特征 | 28 | 64 | 4.07 | 10 | 0 | 3.50 | 64 | 4.06 |
| 筛查工具的获得和使用 | 11 | 64 | 4.13 | 4 | 25 | 3.80 | 73 | 4.24 |
| 医疗服务及社区系统的内部关系 | 28 | 79 | 4.23 | 6 | 17 | 3.75 | 82 | 4.26 |
| 药物治疗选择 | 18 | 78 | 4.20 | 4 | 0 | 3.51 | 78 | 4.19 |
| 双相障碍中的躁狂和抑郁发作 | 4 | 100 | 4.59 | 0 | 0 | 0 | 100 | 4.59 |
| 与患者和社区针对抑郁进行沟通 | 29 | 90 | 4.36 | 3 | 0 | 3.77 | 90 | 4.36 |
| 随访 | 33 | 61 | 4.03 | 13 | 31 | 3.64 | 73 | 4.05 |
| 管理患者信息 | 11 | 82 | 4.20 | 2 | 0 | 3.73 | 82 | 4.20 |
| 指南的整体结构 | 19 | 74 | 4.06 | 5 | 0 | 3.61 | 74 | 4.06 |
| 总体共识 | 199 | 76 | 4.25 | 47 | 13 | 3.66 | 79 | 4.26 |
| 主题 | mhGAP-IG.v2的调整建议 |
|---|---|
| 1."以人为本"的指南 | 1.1不仅是"以患者为中心",而且要强调"以人为本" |
| -确切保护患者隐私 | |
| -对患者的生活事件(如悲伤)保持敏感 | |
| -适应患者的多样性 | |
| 1.2提供个体化的患者管理计划(PMP) | |
| -与患者建立伙伴关系 | |
| -保持随时间发展的灵活性,以满足患者需要 | |
| -列出可以激发出积极的行为改变的几种策略 | |
| 1.3使PMP与医生、患者、业务管理相匹配 | |
| -医生评估治疗进展(如评估药物副作用,改变治疗方法) | |
| -患者对治疗的评价(如对治疗的体验、对治疗的参与) | |
| -业务跟踪(如预约就诊、可能的转诊选项) | |
| 1.4由有心理健康服务证书的全科医生制定PMP框架 | |
| 1.5解决背景不同的问题 | |
| -优先考虑自杀风险 | |
| -在每个服务阶段强调家庭参与 | |
| -提供深圳市患者治疗成功的案例 | |
| 2.双相障碍中的躁狂和抑郁发作 | 2.1区分非复杂抑郁与双相障碍(抑郁发作)在治疗方法上的不同 |
| -把心境稳定剂作为抗抑郁药的辅助用药 | |
| 2.2与患者或家属一起,核查躁狂的症状 | |
| 3.与患者和社区针对抑郁进行沟通 | 3.1医生发挥提高社区意识和健康素养的作用 |
| 3.2更强调家庭在患者支持上的作用 | |
| 3.3将监督有自杀风险患者纳入社区卫生服务中心工作范畴 | |
| 3.4充实患者心理教育的内容 | |
| -纳入培养患者信任的策略(如赋予同理心的倾听) | |
| -纠正任何对疾病的误解 | |
| -提供治疗成功的案例故事 | |
| -让患者准备好应对社区的抑郁污名化 | |
| -讨论治疗依从性的重要性 | |
| -提供参与治疗活动的建议 | |
| -鼓励参加社区卫生服务中心随访和专家随诊 | |
| -与患者达成管理/医疗服务计划的共识 | |
| -提供自我管理的建议 | |
| 3.5考虑实施预约系统 | |
| 4.医疗服务及社区系统的内部关系 | 4.1强调社区参与对自杀风险患者的监督 |
| 4.2明确转诊路径,以及各种职业之间的责任分工 | |
| 4.3强调医学和非医学跨领域服务的机会 | |
| 4.4把家庭参与作为跨领域服务的一部分 | |
| 4.5加上提醒,把患者置于所有讨论的核心 | |
| 5.筛查工具的获得和使用 | 5.1推荐在管理和/或随诊时使用的问卷 |
| 5.2在私密诊室使用问卷 | |
| 5.3医生和护士都能使用问卷(假设提供过培训) | |
| 5.4明确工具范围(多次使用?非临床场所使用?) | |
| 6.管理患者信息 | 6.1看诊前回顾病史,并更新病史记录 |
| 6.2如果需要,补充患者管理系统的信息 | |
| 6.3通过专家、其他治疗医生、家庭成员反馈及评估用药反应等,证实治疗效果 | |
| 6.4定期召开诊所内会议,与其他医生讨论疑难病例 | |
| 7.药物治疗选择 | 7.1在监督和更改药物剂量时,说明医生的任务 |
| 7.2加上每种药物的用药指征和副反应 | |
| 7.3加上每种药物的可得性和医保报销情况 | |
| 7.4加上每种药物的依从建议 | |
| 7.5提供最新药物的详细信息 | |
| 7.6提供药物的商品名举例 | |
| 7.7增加苯二氮 | |
| 8.抑郁障碍的表现特征 | 8.1指南应"反映真实的看诊情况" |
| -考虑患者是否以往有过抑郁发作 | |
| -明确关系问题的细节(包括悲伤) | |
| -在看诊的早期评估患者的自杀风险 | |
| -首先考虑躯体症状 | |
| 8.2包括抑郁的触发因素和风险因素 | |
| 8.3根据"一系列症状,而非核心症状"做出诊断 | |
| -在症状清单中同时列出核心症状和其他症状 | |
| -在症状清单中纳入性欲减退 | |
| -按照是否能更好地预测抑郁/常见症状,列出症状 | |
| -提供随时间变化的症状的额外详细信息 | |
| 8.4在结构上澄清躯体症状和心理症状之间的不同 | |
| 8.5儿童患者需要的额外症状信息 | |
| 8.6谨慎地量化/翻译如下表述 | |
| -"睡眠过多" | |
| -"比平常讲话和活动缓慢" | |
| 9.指南的整体结构 | 9.1为更好地反映应用的背景条件,需要随结构进行某些或较大的重组 |
| 9.2强调跨领域参与,包括家庭/社区网络 | |
| 9.3强调一般抑郁与双相障碍(抑郁发作)之间的不同 | |
| 9.4将随诊和管理整合进一个连续的部分 | |
| 9.5在开始评估时,考虑到高自杀风险患者 | |
| 9.6将患者作为指南的核心 | |
| 10.随访 | 10.1确定随诊,并解释为什么随诊是必要的 |
| -确定患者的治疗状态 | |
| -确定患者以往接受的治疗 | |
| -监测当前治疗的副反应,并评估改善情况 | |
| 10.2解释怎样评估进展,即逐项列出改善的征象 | |
| 10.3强调社区卫生服务中心在随诊中要达到的主要结果 | |
| -在社区卫生服务中心层面,基本心理治疗的选项 | |
| -心理干预/药物治疗的转诊选项 | |
| 10.4逐项列出随诊的联系方式(面对面、电话、电子化) | |
| 10.5推荐首选看诊方式 | |
| -理想的,对所有患者进行面对面随诊 | |
| -至少,对病情严重患者进行面对面随诊 | |
| -患者对非紧急情况的看诊偏好 | |
| 10.6根据抑郁的严重程度、自残风险、治疗依从程度,确定随诊的频率和持续时间 |
Table 2 Primary care recommendations for an adapted mhGAP-IG.v2
| 主题 | mhGAP-IG.v2的调整建议 |
|---|---|
| 1."以人为本"的指南 | 1.1不仅是"以患者为中心",而且要强调"以人为本" |
| -确切保护患者隐私 | |
| -对患者的生活事件(如悲伤)保持敏感 | |
| -适应患者的多样性 | |
| 1.2提供个体化的患者管理计划(PMP) | |
| -与患者建立伙伴关系 | |
| -保持随时间发展的灵活性,以满足患者需要 | |
| -列出可以激发出积极的行为改变的几种策略 | |
| 1.3使PMP与医生、患者、业务管理相匹配 | |
| -医生评估治疗进展(如评估药物副作用,改变治疗方法) | |
| -患者对治疗的评价(如对治疗的体验、对治疗的参与) | |
| -业务跟踪(如预约就诊、可能的转诊选项) | |
| 1.4由有心理健康服务证书的全科医生制定PMP框架 | |
| 1.5解决背景不同的问题 | |
| -优先考虑自杀风险 | |
| -在每个服务阶段强调家庭参与 | |
| -提供深圳市患者治疗成功的案例 | |
| 2.双相障碍中的躁狂和抑郁发作 | 2.1区分非复杂抑郁与双相障碍(抑郁发作)在治疗方法上的不同 |
| -把心境稳定剂作为抗抑郁药的辅助用药 | |
| 2.2与患者或家属一起,核查躁狂的症状 | |
| 3.与患者和社区针对抑郁进行沟通 | 3.1医生发挥提高社区意识和健康素养的作用 |
| 3.2更强调家庭在患者支持上的作用 | |
| 3.3将监督有自杀风险患者纳入社区卫生服务中心工作范畴 | |
| 3.4充实患者心理教育的内容 | |
| -纳入培养患者信任的策略(如赋予同理心的倾听) | |
| -纠正任何对疾病的误解 | |
| -提供治疗成功的案例故事 | |
| -让患者准备好应对社区的抑郁污名化 | |
| -讨论治疗依从性的重要性 | |
| -提供参与治疗活动的建议 | |
| -鼓励参加社区卫生服务中心随访和专家随诊 | |
| -与患者达成管理/医疗服务计划的共识 | |
| -提供自我管理的建议 | |
| 3.5考虑实施预约系统 | |
| 4.医疗服务及社区系统的内部关系 | 4.1强调社区参与对自杀风险患者的监督 |
| 4.2明确转诊路径,以及各种职业之间的责任分工 | |
| 4.3强调医学和非医学跨领域服务的机会 | |
| 4.4把家庭参与作为跨领域服务的一部分 | |
| 4.5加上提醒,把患者置于所有讨论的核心 | |
| 5.筛查工具的获得和使用 | 5.1推荐在管理和/或随诊时使用的问卷 |
| 5.2在私密诊室使用问卷 | |
| 5.3医生和护士都能使用问卷(假设提供过培训) | |
| 5.4明确工具范围(多次使用?非临床场所使用?) | |
| 6.管理患者信息 | 6.1看诊前回顾病史,并更新病史记录 |
| 6.2如果需要,补充患者管理系统的信息 | |
| 6.3通过专家、其他治疗医生、家庭成员反馈及评估用药反应等,证实治疗效果 | |
| 6.4定期召开诊所内会议,与其他医生讨论疑难病例 | |
| 7.药物治疗选择 | 7.1在监督和更改药物剂量时,说明医生的任务 |
| 7.2加上每种药物的用药指征和副反应 | |
| 7.3加上每种药物的可得性和医保报销情况 | |
| 7.4加上每种药物的依从建议 | |
| 7.5提供最新药物的详细信息 | |
| 7.6提供药物的商品名举例 | |
| 7.7增加苯二氮 | |
| 8.抑郁障碍的表现特征 | 8.1指南应"反映真实的看诊情况" |
| -考虑患者是否以往有过抑郁发作 | |
| -明确关系问题的细节(包括悲伤) | |
| -在看诊的早期评估患者的自杀风险 | |
| -首先考虑躯体症状 | |
| 8.2包括抑郁的触发因素和风险因素 | |
| 8.3根据"一系列症状,而非核心症状"做出诊断 | |
| -在症状清单中同时列出核心症状和其他症状 | |
| -在症状清单中纳入性欲减退 | |
| -按照是否能更好地预测抑郁/常见症状,列出症状 | |
| -提供随时间变化的症状的额外详细信息 | |
| 8.4在结构上澄清躯体症状和心理症状之间的不同 | |
| 8.5儿童患者需要的额外症状信息 | |
| 8.6谨慎地量化/翻译如下表述 | |
| -"睡眠过多" | |
| -"比平常讲话和活动缓慢" | |
| 9.指南的整体结构 | 9.1为更好地反映应用的背景条件,需要随结构进行某些或较大的重组 |
| 9.2强调跨领域参与,包括家庭/社区网络 | |
| 9.3强调一般抑郁与双相障碍(抑郁发作)之间的不同 | |
| 9.4将随诊和管理整合进一个连续的部分 | |
| 9.5在开始评估时,考虑到高自杀风险患者 | |
| 9.6将患者作为指南的核心 | |
| 10.随访 | 10.1确定随诊,并解释为什么随诊是必要的 |
| -确定患者的治疗状态 | |
| -确定患者以往接受的治疗 | |
| -监测当前治疗的副反应,并评估改善情况 | |
| 10.2解释怎样评估进展,即逐项列出改善的征象 | |
| 10.3强调社区卫生服务中心在随诊中要达到的主要结果 | |
| -在社区卫生服务中心层面,基本心理治疗的选项 | |
| -心理干预/药物治疗的转诊选项 | |
| 10.4逐项列出随诊的联系方式(面对面、电话、电子化) | |
| 10.5推荐首选看诊方式 | |
| -理想的,对所有患者进行面对面随诊 | |
| -至少,对病情严重患者进行面对面随诊 | |
| -患者对非紧急情况的看诊偏好 | |
| 10.6根据抑郁的严重程度、自残风险、治疗依从程度,确定随诊的频率和持续时间 |
| [1] |
深圳市统计局,深圳市第七次全国人口普查领导小组办公室. 深圳市第七次全国人口普查公报[A/OL]. (2021-05-17)[2022-01-05].
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
中共中央,国务院. "健康中国2030"规划纲要[A/OL]. (2016-10-25)[2022-01-05].
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
WHO. mhGAP intervention guide for mental,neurological and substance use disorders in non-specialized health settings:mental health gap action programme(mhGAP)[M]. Geneva:World Health Organization,2010.
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
WHO. mhGAP intervention guide for mental,neurological and substance use disorder in non-specialised health settings[M]. 2nd ed. Geneva:World Health Organization,2016.
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [42] |
|
| [43] |
|
| [44] |
|
| [45] |
|
| [46] |
|
| [47] |
|
| [48] |
|
| [49] |
|
| [50] |
|
| [51] |
|
| [52] |
|
| [53] |
|
| [54] |
|
| [55] |
|
| [56] |
|
| [57] |
|
| [58] |
|
| [59] |
|
| [60] |
|
| [61] |
|
| [62] |
|
| [63] |
|
| [64] |
|
| [65] |
|
| [66] |
|
| [67] |
|
| [68] |
|
| [69] |
World Health Organization. Framework on integrated,people-centred health services[R]. Geneva:World Health Organization,2016.
|
| [70] |
World Health Organization. Framework on integrated people-centred health services:an overview[EB/OL]. [2022-01-05].
|
| [71] |
|
| [72] |
|
| [73] |
|
| [74] |
|
| [75] |
|
| [76] |
|
| [77] |
|
| [78] |
|
| [79] |
|
| [80] |
|
| [1] | LIAN Lu, CHEN Jiaying, WANG Xuanxuan, LI Yahui, ZHU Ya. Current Situation and Countermeasure of Medical Service Capacity of Primary Care Physicians in China [J]. Chinese General Practice, 2023, 26(34): 4246-4253. |
| [2] | JIAN Qiufeng, XU Ronghua, YAO Qian, ZHOU Yuanyuan. A Meta-analysis of the Prevalence and Influencing Factors of Post-stroke Cognitive Impairment in Chinese Elderly Patients [J]. Chinese General Practice, 2023, 26(32): 4070-4079. |
| [3] | HE Li, ZHANG Yifan, SHEN Xuechun, SUN Yan, ZHAO Yang. Prevalence Trends of Multimorbidity among Residents in Mainland China: a Meta-analysis [J]. Chinese General Practice, 2023, 26(29): 3599-3607. |
| [4] | XU Zhe, ZHANG Jinxia, ZHANG Xiuhong, XIE Kaihong. Relationship between Sleep Duration and All-cause Mortality in Middle-aged and Older Adults [J]. Chinese General Practice, 2023, 26(28): 3507-3512. |
| [5] | GAO Yanli, WANG Hongjun, SUN Fei, JI Xiangqin, Changizi Roohollah. Exploration of Chronic Disease Management Model in Secondary Private General Hospital [J]. Chinese General Practice, 2023, 26(28): 3585-3590. |
| [6] | REN Yanfeng, LIU Shimeng, TAO Ying, CHEN Yingyao. A Systematic Review of Medication Preferences for Patients with Depression Based on Discrete Choice Experiment and Best-worst Scaling [J]. Chinese General Practice, 2023, 26(28): 3559-3564. |
| [7] | LIANG Xuemei, WANG Rui, ZHAO Yuhuan, XU Tianjiao, WANG Wei, SUN Weidong. Transcranial Low-level Laser Therapy: a Novel Treatment for Depression [J]. Chinese General Practice, 2023, 26(27): 3335-3341. |
| [8] | ZHANG Lifeng, ZHANG Ningning, QIN Xiuqun, YANG Yi, ZHONG Dongmei, LIU Shaofei, DAI Yushen, WANG Xiaodan, WANG Mingfei. Healthcare-seeking Behavior and Influencing Factors of Children with Upper Respiratory Tract Infection in the Context of Hierarchical Medical System [J]. Chinese General Practice, 2023, 26(26): 3269-3275. |
| [9] | LI Ziqi, HE Ping, YUAN Beibei, ZHANG Wei, XU Hanyi, WEI Qianchen, MENG Qingyue, XU Jin. Index System Construction and Application Case Analysis for County Health System Development Focusing on Primary Care [J]. Chinese General Practice, 2023, 26(25): 3147-3152. |
| [10] | ZENG Lingfeng, YANG Weiyi, LIANG Guihong, XIAO Xiao, LUO Minghui, PAN Jianke, HAN Yanhong, HUANG Hetao, ZHAO Jinlong, XU Nanjun, ZHOU Guanghui, ZHANG Xianquan, LIANG Weixiong, OU Aihua, LIU Jun, Bone and Joint Professional Committee of Degeneration and Injury of Guangdong Provincial Association of Chinese Medicine. Expert Questionnaire Survey and Result Analysis of TCM Symptom Assessment in High Risk Population of Osteoporosis in Ling-nan Region [J]. Chinese General Practice, 2023, 26(24): 2986-2991. |
| [11] | GUO Yahong, GUO Haoqian, NING Yanhua, JIANG Ting, LI Meiman, LYU Xiongxiong, KONG Weijuan, LIU Haiyan. Construction of "Internet+" Family Nursing Management Model for the Elderly Based on Contracted Family Doctor Services [J]. Chinese General Practice, 2023, 26(23): 2876-2881. |
| [12] | XU Yifan, JING Limei, WANG Lili, WANG Zhaolin, LI Yuhan, LU Wenyuan, ZHANG Qinhua, WANG Haoran, JING Jiaheng, LI Shuijing. Development of a Comprehensive Assessment System of Hospice Care [J]. Chinese General Practice, 2023, 26(22): 2793-2799. |
| [13] | ZHA Qianqian, XU Lianying, CHEN Juan, HUANG Wen, ZHANG Xinqiong. Summary of Best Evidence for Prevention of Recurrence of Late-life Depression [J]. Chinese General Practice, 2023, 26(19): 2332-2338. |
| [14] | WANG Ping, ZHOU Qi, ZHAO Junxian, WU Shouyuan, SUN Yajia, LAN Hui, REN Mengjuan, SU Renfeng, WANG Ling, WANG Qi, LI Sheyu, HUANG Yanli, WANG Xiaohui, MA Yanfang, MA Li, XU Yanli, SUN Yange, SHI Ling, HUANG Yanyan, HOU Tianchun, GE Long, DU Zhaohui, ZHENG Yanling, YIN Zhaoxia, LI Tingting, ZENG Linan, ZHANG Xiaolong, REN Yanping, LIU Enmei, YI Chuntao, CHEN Yaolong. Development of Reporting Items for Practice Guidelines in Primary Care [J]. Chinese General Practice, 2023, 26(13): 1543-1550. |
| [15] | WANG Ping, WU Shouyuan, SUN Yajia, LAN Hui, REN Mengjuan, ZHAO Junxian, WANG Ling, SU Renfeng, ZHOU Qi, WANG Zijun, WANG Qi, MA Li, HOU Tianchun, CHEN Yaolong. Current Situation Analysis and Quality Evaluation of Chinese Clinical Practice Guidelines in General Practice [J]. Chinese General Practice, 2023, 26(13): 1551-1558. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||