中国全科医学 ›› 2024, Vol. 27 ›› Issue (24): 2976-2981.DOI: 10.12114/j.issn.1007-9572.2023.0679
和军辉, 万大国*( ), 董静, 张娟
), 董静, 张娟
HE Junhui, WAN Daguo*(), DONG Jing, ZHANG Juan
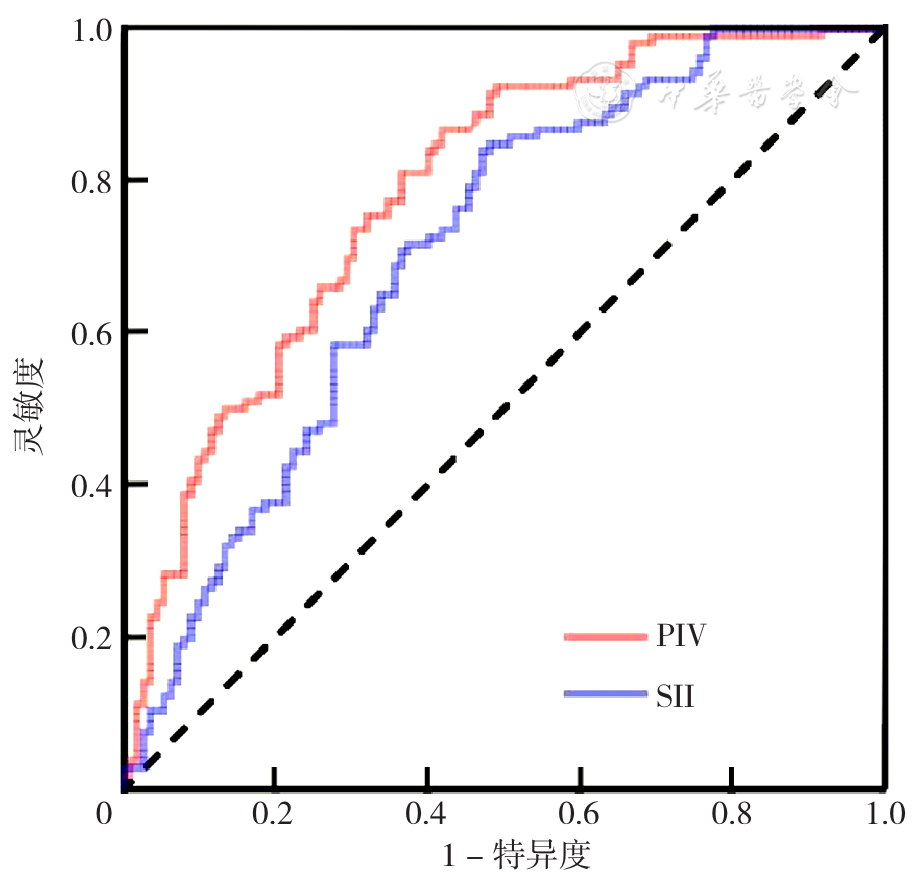
摘要: 背景 泛免疫炎症值(PIV)、全身免疫炎症指数(SII)被认为是评估动脉粥样硬化性心血管疾病风险的新型炎症指标,然而较少有研究探讨PIV、SII对动脉粥样硬化斑块的影响。 目的 通过光学相干断层成像技术(OCT)探讨急性冠脉综合征(ACS)患者PIV、SII与冠状动脉粥样硬化易损斑块的关系。 方法 回顾性纳入2020年12月—2023年6月就诊于郑州大学第二附属医院心内科的ACS患者525例为研究对象,患者均接受冠状动脉造影及OCT检查,根据薄纤维帽粥样硬化斑块(TFCA)诊断标准分为非TCFA组(112例)和TCFA组(106例)。收集资料并进行分析。采用多因素有序Logistic回归分析探究TCFA的影响因素。绘制PIV、SII诊断TCFA的受试者工作特征曲线(ROC曲线),计算ROC曲线下面积(AUC)。基于PIV的最佳截断值将患者分为低PIV组(PIV<337.86,79例)和高PIV组(PIV≥337.86,139例),同时基于SII的最佳截断值将患者分为低SII组(SII<775.63,74例)和高SII组(SII≥775.63,144例)。 结果 TCFA组高血压、糖尿病比例、泛PIV、SII、C反应蛋白(CRP)、有吸烟史比例、术前收缩压高于非TCFA组(P<0.05)。多因素Logistic回归分析结果显示PIV(OR=1.015,95%CI=1.010~1.020,P<0.001)、SII(OR=1.005,95%CI=1.003~1.007,P<0.001)为发生TCFA的危险因素。ROC曲线结果显示PIV、SII诊断TCFA的AUC分别为0.785(95%CI=0.725~0.845,P<0.001)、0.707(95%CI=0.639~0.776,P<0.001)。高PIV组巨噬细胞浸润、点状钙化、易损斑块比例高于低PIV组(P<0.05);高SII组巨噬细胞浸润、微通道、易损斑块比例高于低SII组(P<0.05)。高PIV组纤维帽厚度低于低PIV组,最大脂质斑块角、平均脂质斑块角度、脂质斑块长度、脂质指数高于低PIV组(P<0.05),高SII组纤维帽厚度低于低SII组,最大脂质斑块角、平均脂质斑块角度、脂质斑块长度、脂质指数高于低SII组(P<0.05)。 结论 高水平PIV、SII可能与ACS患者易损斑块的发生率相关。PIV、SII水平在评估ACS患者冠状动脉粥样硬化易损斑块特征及易损性方面具有一定价值。