中国全科医学 ›› 2024, Vol. 27 ›› Issue (32): 3987-3992.DOI: 10.12114/j.issn.1007-9572.2024.0047
吕广瑜1,2, 孙宛君3, 周倩倩1, 陈先梦1, 刘雪晗4, 胡晓文1,*( )
)
LYU Guangyu1,2, SUN Wanjun3, ZHOU Qianqian1, CHEN Xianmeng1, LIU Xuehan4, HU Xiaowen1,*()
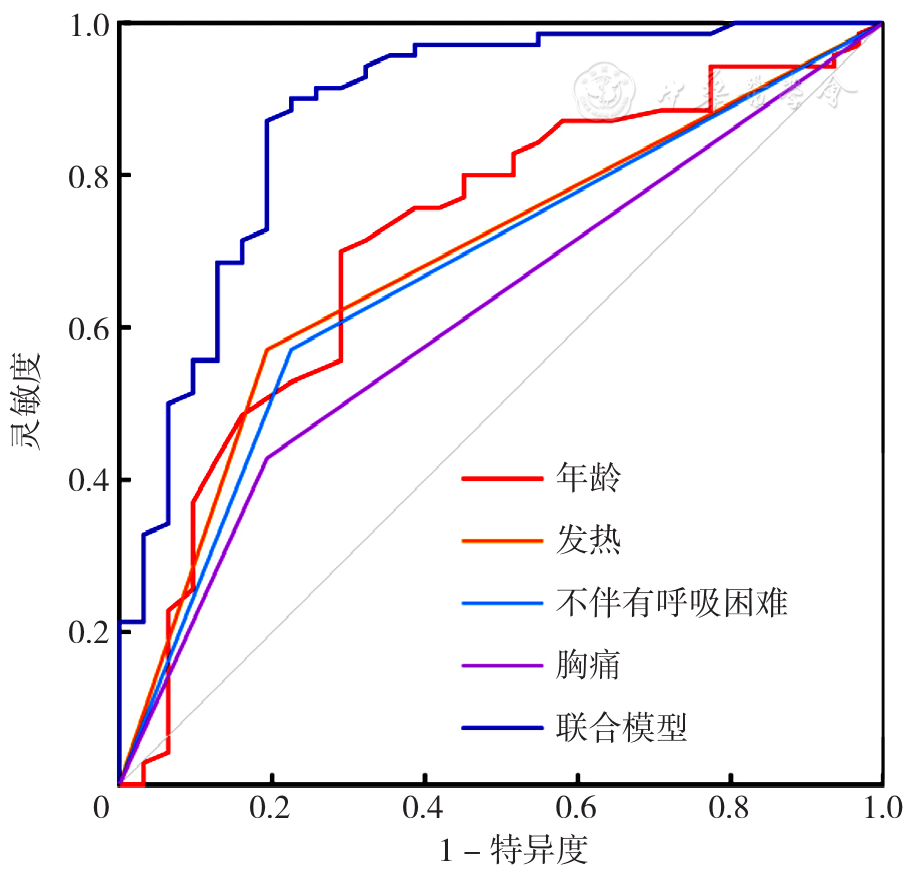
摘要: 背景 尽管近年来肺栓塞继发肺梗死的病例不断见诸报道,但该病的误诊仍较普遍,其中最常被误诊为肺炎,尤其是存在中高危风险患者,延迟诊断、未能及时接受治疗将会影响患者的预后。 目的 总结中高危肺栓塞继发肺梗死被误诊为肺炎患者的临床特征,分析相关危险因素,并构建早期诊断模型。 方法 回顾性收集中国科学技术大学附属第一医院2017—2023年确诊为中高危风险肺栓塞继发肺梗死的住院患者临床资料。分析患者误诊情况,根据诊断情况分为误诊组(曾误诊为肺炎离院回家)和对照组(门诊或急诊科首次就诊即正确诊断)。采用多因素二元Logistic回归分析探究中高危风险肺栓塞继发肺梗死被误诊为肺炎的影响因素,绘制受试者工作特征曲线(ROC曲线)分析各指标对中高危风险肺栓塞继发肺梗死被误诊为肺炎的预测价值,并采用Delong检验比较各ROC曲线下面积(AUC)。 结果 共纳入患者101例,其中70例中高危肺栓塞继发肺梗死患者被误诊为肺炎。2017—2023年中高危肺栓塞继发肺梗死患者被误诊为肺炎的发生率呈下降趋势(依次为100.0%、83.3%、74.1%、71.4%、63.2%、66.7%、50.0%,χ2趋势=6.672,P=0.010)。多因素二元Logistic回归分析结果显示,年龄≥60岁(OR=18.271,95%CI=4.373~76.339,P<0.001)、发热(OR=16.073,95%CI=3.510~73.786,P<0.001)、胸痛(OR=6.660,95%CI=1.571~28.233,P=0.010)和不伴有呼吸困难(OR=7.783,95%CI=2.049~30.249,P=0.003)是中高危风险肺栓塞继发肺梗死被误诊为肺炎的独立影响因素。经筛选得出,多变量联合模型=-6.624+0.095×年龄+2.510×发热+2.683×不伴有呼吸困难,联合模型预测中高危风险肺栓塞继发肺梗死被误诊为肺炎的AUC为0.880(95%CI=0.802~0.959),灵敏度为0.871,特异度为0.806。Delong检验结果显示,联合模型预测价值优于单因素指标如年龄(Z=2.771,P=0.006)、发热(Z=4.653,P<0.001)及不伴有呼吸困难(Z=4.014,P<0.001)。 结论 尽管2017—2023年中高危肺栓塞继发肺梗死患者被误诊为肺炎的比例有所降低,但当老年肺栓塞患者出现发热、胸痛并且不伴有呼吸困难时,临床医生应注意肺梗死与肺炎的鉴别诊断。
中图分类号: