Background Thyroid dysfunction is common in patients with coronary artery disease (CAD) following percutaneous coronary intervention (PCI). However, its impact on cardiac structure and function within the context of chronic comorbidities remains unclear.
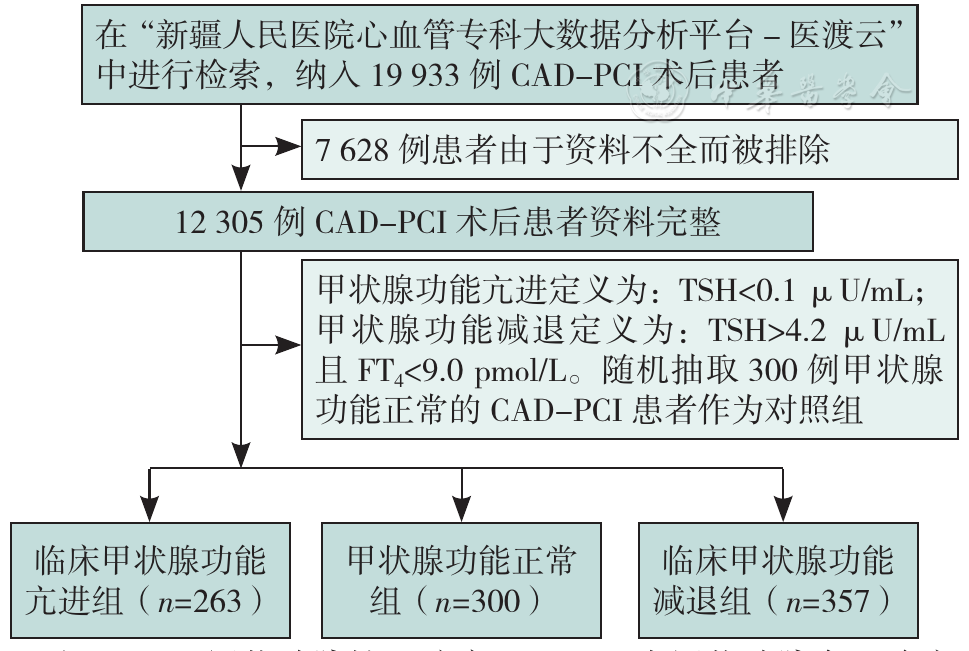
Methods Data were sourced from the "Xinjiang People's Hospital Cardiovascular Specialty Big Data Analysis Platform-Yidu Cloud" including clinical data of CAD patients post-PCI from 2013 to 2022. Thyroid function, echocardiography, and biochemical indices were measured. Patients were classified based on diagnostic criteria into clinical hyperthyroidism group (n=263), clinical hypothyroidism group (n=357), and a control group of euthyroid patients (n=300). Spearman rank correlation was used to explore the relationship between thyroid function and cardiac structure/function. Multivariate Logistic regression and unconditional multivariate Logistic regression analyses were conducted to investigate factors affecting cardiac systolic and diastolic dysfunction. Receiver operating characteristic (ROC) curves were plotted to determine the diagnostic value of thyroid function indices for cardiac dysfunction and to calculate the area under the ROC curve (AUC) .
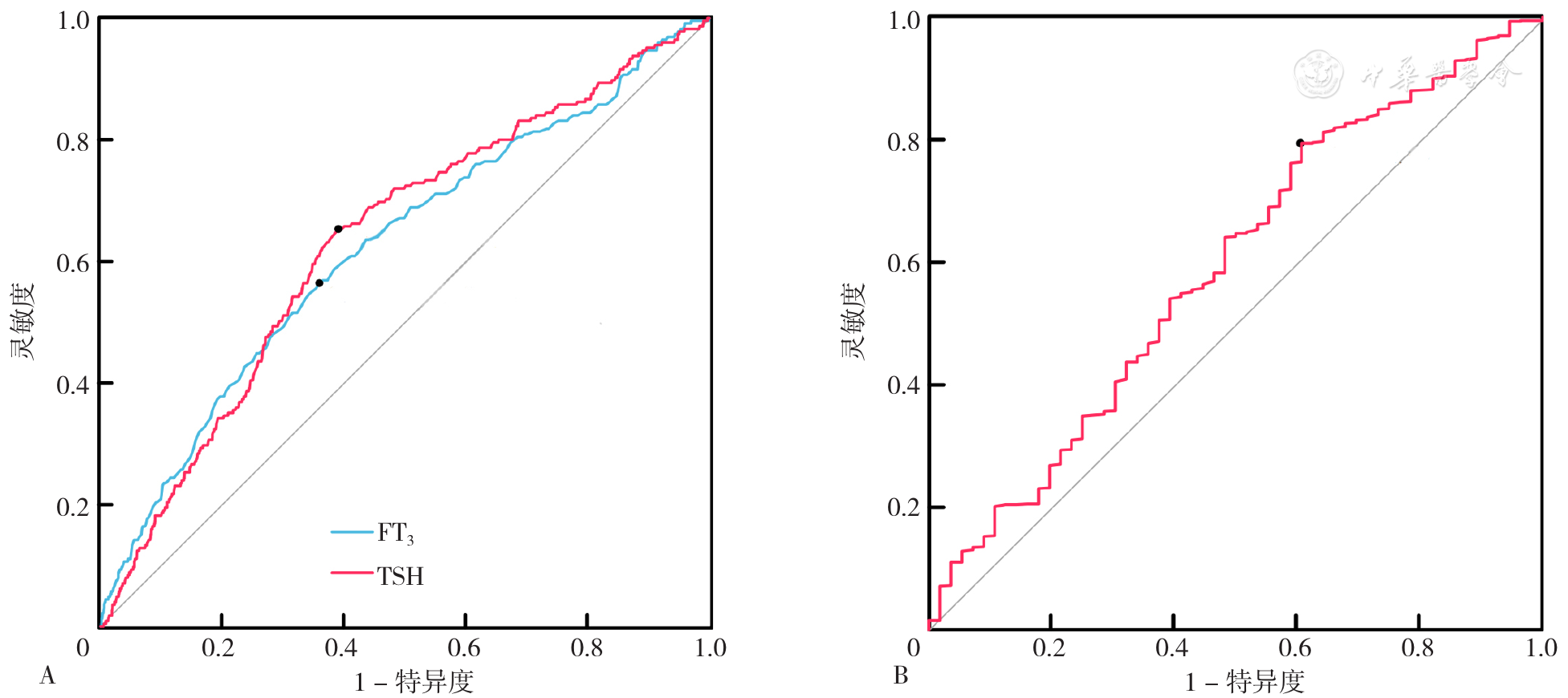
Results Significant differences were observed among the three groups in age, gender, diastolic blood pressure (DBP), systolic blood pressure (SBP), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), cystatin C (CysC), alanine aminotransferase (ALT), aspartate aminotransferase (AST), B-type natriuretic peptide (BNP), fasting glucose (GLU), lipoprotein (a) (LPa), thyroxine (T4), free thyroxine (FT4), triiodothyronine (T3), free triiodothyronine (FT3), thyroid-stimulating hormone (TSH), thyroglobulin antibody (TgAb), and thyroid peroxidase antibody (TPOAb) (P<0.05). Significant differences were also found in aortic diameter (AOd), right ventricular diameter (RVd), left ventricular end-diastolic diameter (LVDd), left ventricular end-systolic diameter (LVSd), left ventricular end-diastolic volume (LVEDV), left ventricular ejection fraction (LVEF), and stroke volume (SV) (P<0.05). Spearman rank correlation analysis showed positive correlations of LVEF with FT3, T3, and TSH (P<0.05) ; AOd with FT3 and T3, and negative correlations with TgAb and TSH (P<0.05) ; LVDd with FT3, and negative correlations with TgAb and TSH (P<0.05) ; LVSd with FT3, T3, T4, and TSH (P<0.05) ; SV with FT3, T3, and negative correlation with TgAb (P<0.05) ; RVd with FT3, and negative correlation with TSH (P<0.05) ; interventricular septal thickness (IVSd) with TgAb (P<0.05) ; LVEDV with FT3, and negative correlations with TgAb and TSH (P<0.05) ; left ventricular posterior wall thickness (LVPWd) with TgAb (P<0.05). Multivariate Logistic regression indicated that FT3 and TSH were factors affecting cardiac systolic dysfunction (P<0.05), while T4 influenced cardiac diastolic dysfunction (P<0.05). ROC curve analysis revealed that the AUCs for predicting cardiac systolic dysfunction were 0.621 (95%CI=0.581-0.662) for FT3 and 0.632 (95%CI=0.594-0.670) for TSH; for predicting cardiac diastolic dysfunction, the AUC for T4 was 0.590 (95%CI=0.510-0.670). Stratified analysis indicated no significant differences in the impact of FT3 on cardiac systolic dysfunction between different ages and genders (Ptrend>0.05), whereas TSH showed differences (Ptrend<0.05). The protective effects of FT3 and TSH on cardiac systolic function were more significant in females and individuals aged≥60 years (P<0.05). The influence of T4 on cardiac diastolic dysfunction differed by age and gender (Ptrend<0.05) .
Conclusion Thyroid dysfunction significantly affects cardiac structure and function in CAD patients post-PCI. FT3 and TSH primarily influence cardiac systolic function, while T4 mainly affects diastolic function. Greater attention should be given to the impact of thyroid function on cardiac function in females and individuals aged<60 years to prevent diastolic dysfunction and high-output low-resistance heart failure.

 )
)