
中国全科医学 ›› 2024, Vol. 27 ›› Issue (24): 2954-2960.DOI: 10.12114/j.issn.1007-9572.2023.0793
祁海燕1, 王捷2, 罗玉玺3, 武云1,*( )
)
收稿日期:2023-09-13
修回日期:2024-03-01
出版日期:2024-08-20
发布日期:2024-05-08
通讯作者:
武云
作者贡献:
祁海燕进行数据收集、结果分析与解释、统计学处理与论文撰写;王捷进行研究方法指导及质量控制;罗玉玺进行数据二次核对;武云进行文章构思、可行性分析及审校,对文章整体监督管理。
基金资助:
QI Haiyan1, WANG Jie2, LUO Yuxi3, WU Yun1,*()
Received:2023-09-13
Revised:2024-03-01
Published:2024-08-20
Online:2024-05-08
Contact:
WU Yun
摘要: 背景 近年来众多研究表明高尿酸血症(HUA)是某些疾病的影响因素,然而HUA是否为慢性肺源性心脏病(CPHD)的影响因素仍需进一步研究。 目的 探讨HUA与CPHD的相关性,旨在为CPHD患者血尿酸(SUA)水平的管理提供理论依据。 方法 纳入2019—2023年新疆医科大学第一附属医院收治的1 171例慢性阻塞性肺疾病(COPD)患者为研究对象,根据其是否患有CPHD分为CPHD组(470例)和COPD组(701例)。收集患者一般资料和实验室检查及超声心动图检查结果。采用LASSO回归法对变量进行筛选,采用倾向性评分匹配法(PSM)排除混杂因素影响。采用多因素Logistic回归分析探究COPD患者合并CPHD的影响因素。 结果 CPHD组女性、汉族、吸烟、饮酒、特发性肺纤维化、慢性支气管炎、支气管哮喘比例、淋巴细胞百分比、左心室舒张末期内径、左心室收缩末期内径、心输出量、左心室射血分数低于COPD组,心功能3~4级、HUA、肺栓塞、先天性心脏病比例、红细胞计数、中性粒细胞百分比、SUA、血尿素氮、D-二聚体、N末端-B型利钠肽前体、右心房内径、右心室内径、左心房内径、右心室流出道内径、肺动脉内径高于COPD组,差异有统计学意义(P<0.05)。LASSO回归筛选出变量后进行PSM,最终得到COPD组469例、CPHD组469例。匹配后CPHD组心功能3~4级、HUA占比、右心房内径、右心室内径、右心室流出道内径、肺动脉内径大于COPD组,支气管哮喘、淋巴细胞百分比低于COPD组,差异有统计学意义(P<0.05)。多因素Logistic回归分析结果显示,HUA升高、心功能3~4级、右心房内径、右心室内径、肺动脉内径增加是COPD患者合并CPHD的危险因素(P<0.05),患有支气管哮喘、左心室舒张末期内径增加为COPD患者合并CPHD的保护因素(P<0.05)。将SUA水平按四分位数分层,多因素Logistic回归分析结果显示,与Q1(SUA<237.31 μmol/L)比较,Q4(SUA>381.29 μmol/L)患者患有CPHD的风险增加1.421倍。 结论 HUA是CPHD疾病发生、发展的影响因素,积极控制SUA水平有助于预防CPHD的发生、发展。
| 项目 | COPD组(n=701) | CPHD组(n=470) | χ2(Z)值 | P值 |
|---|---|---|---|---|
| 性别(男/女) | 445/256 | 258/212 | 8.647 | 0.003 |
| 年龄[例(%)] | 2.412 | 0.491 | ||
| 20~39岁 | 4(0.5) | 3(0.6) | ||
| 40~59岁 | 124(17.7) | 69(14.7) | ||
| 60~79岁 | 417(59.5) | 281(59.8) | ||
| 80~99岁 | 156(22.3) | 117(24.9) | ||
| 民族[例(%)] | 23.406 | <0.001 | ||
| 少数民族 | 258(36.8) | 240(51.1) | ||
| 汉族 | 443(63.2) | 230(48.9) | ||
| 吸烟[例(%)] | 11.891 | 0.001 | ||
| 否 | 465(66.3) | 356(75.7) | ||
| 是 | 236(33.7) | 114(24.3) | ||
| 饮酒[例(%)] | 36.692 | <0.001 | ||
| 否 | 492(70.2) | 402(85.5) | ||
| 是 | 209(29.8) | 68(14.5) | ||
| 心功能[例(%)] | 195.541 | <0.001 | ||
| 2级以下 | 632(90.2) | 256(54.5) | ||
| 3~4级 | 69(9.8) | 214(45.5) | ||
| HUA[例(%)] | 86.266 | <0.001 | ||
| 无 | 637(90.9) | 328(69.8) | ||
| 有 | 64(9.1) | 142(30.2) | ||
| 高血压[例(%)] | 0.013 | 0.908 | ||
| 无 | 338(48.2) | 225(47.9) | ||
| 有 | 363(51.8) | 245(52.1) | ||
| 糖尿病[例(%)] | 0.278 | 0.598 | ||
| 无 | 552(78.7) | 364(77.4) | ||
| 有 | 149(21.3) | 106(22.6) | ||
| 冠心病[例(%)] | 3.750 | 0.053 | ||
| 无 | 542(77.3) | 340(72.3) | ||
| 有 | 159(22.7) | 130(27.7) | ||
| 抑郁症[例(%)] | 0.244 | 0.621 | ||
| 无 | 698(99.6) | 467(99.4) | ||
| 有 | 3(0.4) | 3(0.6) | ||
| 焦虑症[例(%)] | 2.657 | 0.103 | ||
| 无 | 698(99.6) | 464(98.7) | ||
| 有 | 3(0.4) | 6(1.3) | ||
| OSAHS[例(%)] | 1.138 | 0.286 | ||
| 无 | 638(91) | 436(92.8) | ||
| 有 | 63(9) | 34(7.2) | ||
| 肺栓塞[例(%)] | 7.449 | 0.006 | ||
| 无 | 671(95.7) | 432(91.9) | ||
| 有 | 30(4.3) | 38(8.1) | ||
| 特发性肺纤维化[例(%)] | 5.407 | 0.020 | ||
| 无 | 627(89.4) | 439(93.4) | ||
| 有 | 74(10.6) | 31(6.6) | ||
| 慢性支气管炎[例(%)] | 6.023 | 0.014 | ||
| 无 | 600(85.6) | 425(90.4) | ||
| 有 | 101(14.4) | 45(9.6) | ||
| 支气管扩张[例(%)] | 0.113 | 0.737 | ||
| 无 | 603(86.0) | 401(85.3) | ||
| 有 | 98(14.0) | 69(14.7) | ||
| 肺部感染[例(%)] | 3.552 | 0.059 | ||
| 无 | 369(52.6) | 221(47.0) | ||
| 有 | 332(47.4) | 249(53.0) | ||
| 肺动脉瓣疾病[例(%)] | 2.988 | 0.084 | ||
| 无 | 701(100.0) | 468(99.6) | ||
| 有 | 0 | 2(0.4) | ||
| 先天性心脏病[例(%)] | 5.348 | 0.021 | ||
| 无 | 699(99.7) | 463(98.5) | ||
| 有 | 2(0.3) | 7(1.5) | ||
| 支气管哮喘[例(%)] | 26.469 | <0.001 | ||
| 无 | 494(70.5) | 393(83.6) | ||
| 有 | 207(29.5) | 77(16.4) | ||
| BMI[M(P25,P75),kg/m2] | 24.7(22.0,27.0) | 24.7(21.0,26.0) | -0.512a | 0.609 |
| RBC[M(P25,P75),×1012/L] | 4.5(4.0,4.9) | 4.8(4.2,5.4) | -5.981a | <0.001 |
| WBC[M(P25,P75),×109/L] | 7.0(5.6,9.1) | 7.1(5.6,8.5) | -0.149a | 0.882 |
| 中性粒细胞百分比[M(P25,P75),%] | 66.7(58.1,77.3) | 71.9(63.7,80.0) | -6.174a | <0.001 |
| 淋巴细胞百分比[M(P25,P75),%] | 21.9(13.6,29.7) | 16.6(10.6,22.8) | -7.167a | <0.001 |
| SUA[M(P25,P75),μmol/L] | 288.9(232.9,358.4) | 316.6(245.6,441.5) | -6.020a | <0.001 |
| Scr[M(P25,P75),μmol/L] | 66.1(55.4,79.1) | 63.5(52.8,78.6) | -1.336a | 0.182 |
| BUN[M(P25,P75),mmol/L] | 5.9(4.6,7.1) | 6.3(5.0,8.4) | -4.674a | <0.001 |
| D-二聚体[M(P25,P75),ng/mL] | 206.0(114.0,421.5) | 367.5(180.8,724.8) | -8.408a | <0.001 |
| NT-proBNP[M(P25,P75),ng/L] | 168(63,851) | 1 550(360,3 335) | -15.206a | <0.001 |
| 右心房内径[M(P25,P75),mm] | 33(32,35) | 43(36,46) | -20.520a | <0.001 |
| 右心室内径[M(P25,P75),mm] | 19(18,20) | 24(20,27) | -18.591a | <0.001 |
| 左心房内径[M(P25,P75),mm] | 34(32,36) | 36(33,40) | -7.100a | <0.001 |
| 左心室舒张末期内径[M(P25,P75),mm] | 48(45,49) | 47(43,50) | -3.920a | <0.001 |
| 左心室收缩末期内径[M(P25,P75),mm] | 32(30,33) | 31(28,33) | -2.176a | 0.030 |
| 右心室流出道内径[M(P25,P75),mm] | 28(26,30) | 34(30,38) | -17.739a | <0.001 |
| 肺动脉内径[M(P25,P75),mm] | 24(22,25) | 30(26,32) | -18.832a | <0.001 |
| EA[M(P25,P75)] | 0.8(0.7,1.1) | 0.8(0.7,0.9) | -0.043a | 0.966 |
| CO[M(P25,P75),L/min] | 4.9(4.4,5.6) | 4.8(4.0,5.7) | -3.218a | 0.001 |
| EF[M(P25,P75),%] | 62.4(61.0,64.0) | 61.9(63.7,69.9) | -5.279a | <0.001 |
表1 CPHD组与COPD组患者一般资料比较
Table 1 Comparison of general data between CPHD group and COPD group
| 项目 | COPD组(n=701) | CPHD组(n=470) | χ2(Z)值 | P值 |
|---|---|---|---|---|
| 性别(男/女) | 445/256 | 258/212 | 8.647 | 0.003 |
| 年龄[例(%)] | 2.412 | 0.491 | ||
| 20~39岁 | 4(0.5) | 3(0.6) | ||
| 40~59岁 | 124(17.7) | 69(14.7) | ||
| 60~79岁 | 417(59.5) | 281(59.8) | ||
| 80~99岁 | 156(22.3) | 117(24.9) | ||
| 民族[例(%)] | 23.406 | <0.001 | ||
| 少数民族 | 258(36.8) | 240(51.1) | ||
| 汉族 | 443(63.2) | 230(48.9) | ||
| 吸烟[例(%)] | 11.891 | 0.001 | ||
| 否 | 465(66.3) | 356(75.7) | ||
| 是 | 236(33.7) | 114(24.3) | ||
| 饮酒[例(%)] | 36.692 | <0.001 | ||
| 否 | 492(70.2) | 402(85.5) | ||
| 是 | 209(29.8) | 68(14.5) | ||
| 心功能[例(%)] | 195.541 | <0.001 | ||
| 2级以下 | 632(90.2) | 256(54.5) | ||
| 3~4级 | 69(9.8) | 214(45.5) | ||
| HUA[例(%)] | 86.266 | <0.001 | ||
| 无 | 637(90.9) | 328(69.8) | ||
| 有 | 64(9.1) | 142(30.2) | ||
| 高血压[例(%)] | 0.013 | 0.908 | ||
| 无 | 338(48.2) | 225(47.9) | ||
| 有 | 363(51.8) | 245(52.1) | ||
| 糖尿病[例(%)] | 0.278 | 0.598 | ||
| 无 | 552(78.7) | 364(77.4) | ||
| 有 | 149(21.3) | 106(22.6) | ||
| 冠心病[例(%)] | 3.750 | 0.053 | ||
| 无 | 542(77.3) | 340(72.3) | ||
| 有 | 159(22.7) | 130(27.7) | ||
| 抑郁症[例(%)] | 0.244 | 0.621 | ||
| 无 | 698(99.6) | 467(99.4) | ||
| 有 | 3(0.4) | 3(0.6) | ||
| 焦虑症[例(%)] | 2.657 | 0.103 | ||
| 无 | 698(99.6) | 464(98.7) | ||
| 有 | 3(0.4) | 6(1.3) | ||
| OSAHS[例(%)] | 1.138 | 0.286 | ||
| 无 | 638(91) | 436(92.8) | ||
| 有 | 63(9) | 34(7.2) | ||
| 肺栓塞[例(%)] | 7.449 | 0.006 | ||
| 无 | 671(95.7) | 432(91.9) | ||
| 有 | 30(4.3) | 38(8.1) | ||
| 特发性肺纤维化[例(%)] | 5.407 | 0.020 | ||
| 无 | 627(89.4) | 439(93.4) | ||
| 有 | 74(10.6) | 31(6.6) | ||
| 慢性支气管炎[例(%)] | 6.023 | 0.014 | ||
| 无 | 600(85.6) | 425(90.4) | ||
| 有 | 101(14.4) | 45(9.6) | ||
| 支气管扩张[例(%)] | 0.113 | 0.737 | ||
| 无 | 603(86.0) | 401(85.3) | ||
| 有 | 98(14.0) | 69(14.7) | ||
| 肺部感染[例(%)] | 3.552 | 0.059 | ||
| 无 | 369(52.6) | 221(47.0) | ||
| 有 | 332(47.4) | 249(53.0) | ||
| 肺动脉瓣疾病[例(%)] | 2.988 | 0.084 | ||
| 无 | 701(100.0) | 468(99.6) | ||
| 有 | 0 | 2(0.4) | ||
| 先天性心脏病[例(%)] | 5.348 | 0.021 | ||
| 无 | 699(99.7) | 463(98.5) | ||
| 有 | 2(0.3) | 7(1.5) | ||
| 支气管哮喘[例(%)] | 26.469 | <0.001 | ||
| 无 | 494(70.5) | 393(83.6) | ||
| 有 | 207(29.5) | 77(16.4) | ||
| BMI[M(P25,P75),kg/m2] | 24.7(22.0,27.0) | 24.7(21.0,26.0) | -0.512a | 0.609 |
| RBC[M(P25,P75),×1012/L] | 4.5(4.0,4.9) | 4.8(4.2,5.4) | -5.981a | <0.001 |
| WBC[M(P25,P75),×109/L] | 7.0(5.6,9.1) | 7.1(5.6,8.5) | -0.149a | 0.882 |
| 中性粒细胞百分比[M(P25,P75),%] | 66.7(58.1,77.3) | 71.9(63.7,80.0) | -6.174a | <0.001 |
| 淋巴细胞百分比[M(P25,P75),%] | 21.9(13.6,29.7) | 16.6(10.6,22.8) | -7.167a | <0.001 |
| SUA[M(P25,P75),μmol/L] | 288.9(232.9,358.4) | 316.6(245.6,441.5) | -6.020a | <0.001 |
| Scr[M(P25,P75),μmol/L] | 66.1(55.4,79.1) | 63.5(52.8,78.6) | -1.336a | 0.182 |
| BUN[M(P25,P75),mmol/L] | 5.9(4.6,7.1) | 6.3(5.0,8.4) | -4.674a | <0.001 |
| D-二聚体[M(P25,P75),ng/mL] | 206.0(114.0,421.5) | 367.5(180.8,724.8) | -8.408a | <0.001 |
| NT-proBNP[M(P25,P75),ng/L] | 168(63,851) | 1 550(360,3 335) | -15.206a | <0.001 |
| 右心房内径[M(P25,P75),mm] | 33(32,35) | 43(36,46) | -20.520a | <0.001 |
| 右心室内径[M(P25,P75),mm] | 19(18,20) | 24(20,27) | -18.591a | <0.001 |
| 左心房内径[M(P25,P75),mm] | 34(32,36) | 36(33,40) | -7.100a | <0.001 |
| 左心室舒张末期内径[M(P25,P75),mm] | 48(45,49) | 47(43,50) | -3.920a | <0.001 |
| 左心室收缩末期内径[M(P25,P75),mm] | 32(30,33) | 31(28,33) | -2.176a | 0.030 |
| 右心室流出道内径[M(P25,P75),mm] | 28(26,30) | 34(30,38) | -17.739a | <0.001 |
| 肺动脉内径[M(P25,P75),mm] | 24(22,25) | 30(26,32) | -18.832a | <0.001 |
| EA[M(P25,P75)] | 0.8(0.7,1.1) | 0.8(0.7,0.9) | -0.043a | 0.966 |
| CO[M(P25,P75),L/min] | 4.9(4.4,5.6) | 4.8(4.0,5.7) | -3.218a | 0.001 |
| EF[M(P25,P75),%] | 62.4(61.0,64.0) | 61.9(63.7,69.9) | -5.279a | <0.001 |
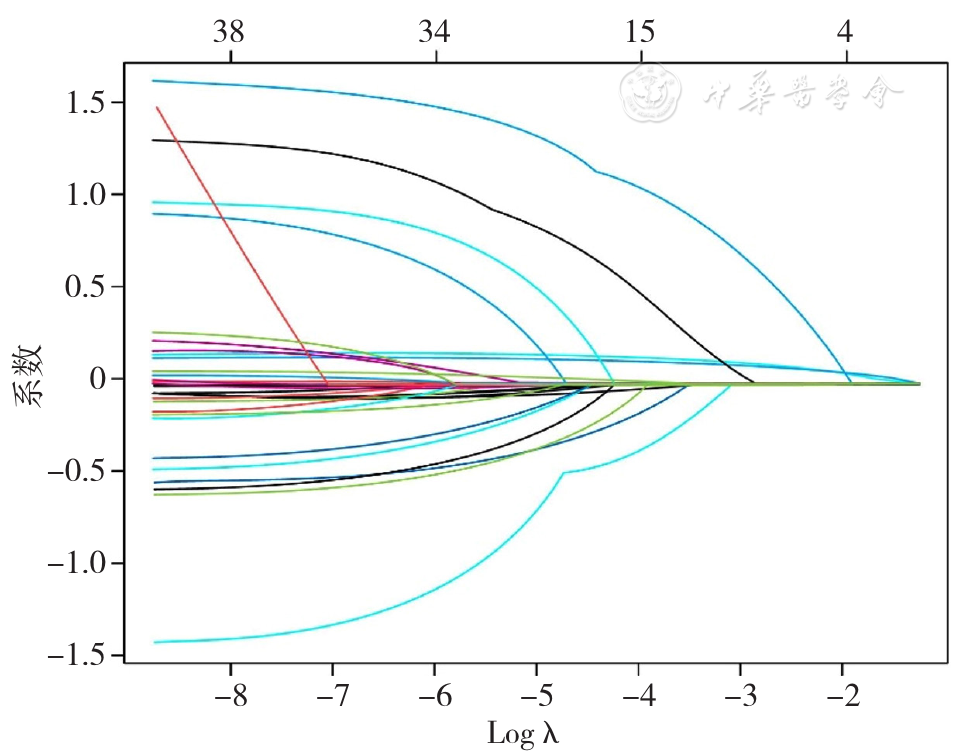
图1 LASSO模型回归系数轨迹图
Figure 1 LASSO model regression coefficient trajectory plot
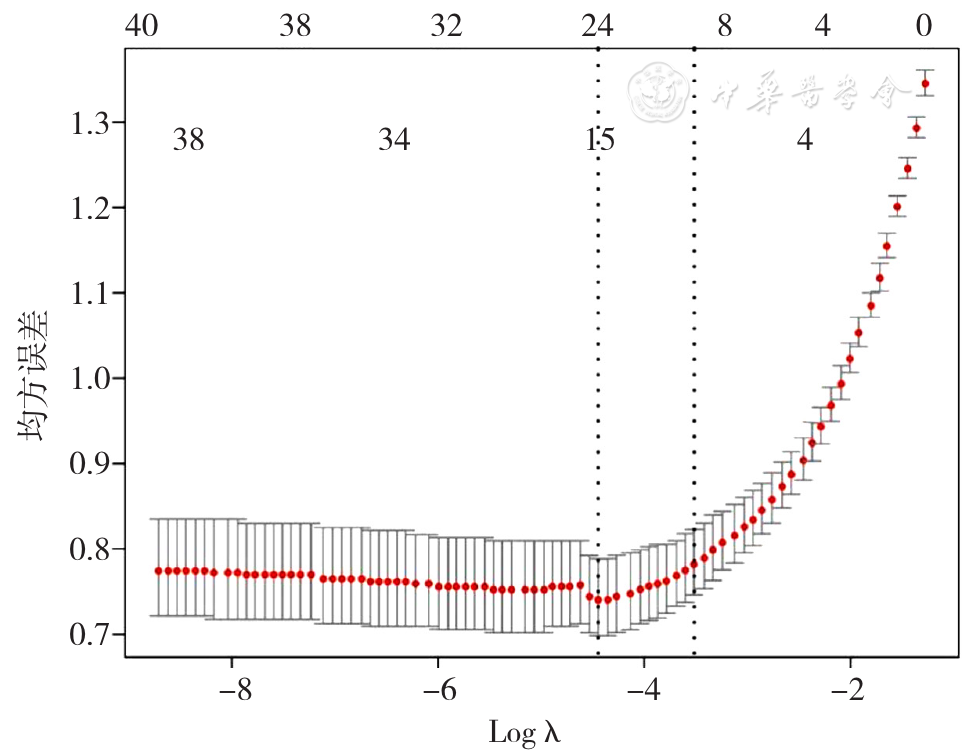
图2 LASSO回归模型中的最佳惩罚系数λ的变化图
Figure 2 Change plot of the optimal penalty coefficient λ in the LASSO regression model
| 项目 | COPD组(n=469) | CPHD组(n=469) | Z(χ2)值 | P值 |
|---|---|---|---|---|
| 年龄[例(%)] | <0.001a | >0.999 | ||
| 20~39岁 | 2(0.4) | 2(0.4) | ||
| 40~59岁 | 69(14.7) | 69(14.7) | ||
| 60~79岁 | 281(59.9) | 281(59.9) | ||
| 80~99岁 | 117(25.0) | 117(25.0) | ||
| 饮酒[例(%)] | <0.001a | >0.999 | ||
| 无 | 401(85.5) | 401(85.5) | ||
| 有 | 68(14.5) | 68(14.5) | ||
| 心功能[例(%)] | 150.182a | <0.001 | ||
| 2级以下 | 423(90.2) | 255(54.4) | ||
| 3~4级 | 46(9.8) | 214(45.6) | ||
| HUA[例(%)] | 73.246a | <0.001 | ||
| 无 | 431(91.9) | 328(69.9) | ||
| 有 | 38(8.1) | 141(30.1) | ||
| 支气管哮喘[例(%)] | 22.602a | <0.001 | ||
| 无 | 332(70.8) | 393(83.8) | ||
| 有 | 137(29.2) | 76(16.2) | ||
| 淋巴细胞百分比[M(P25,P75),%] | 22.0(13.8,29.9) | 16.6(10.6,22.8) | -6.802 | <0.001 |
| 右心房内径[M(P25,P75),mm] | 33(32,35) | 42(36,46) | -18.863 | <0.001 |
| 右心室内径[M(P25,P75),mm] | 19(18,20) | 24(20,27) | -17.177 | <0.001 |
| 左心室舒张末期内径[M(P25,P75),mm] | 47(45,49) | 47(43,50) | -3.349 | <0.001 |
| 右心室流出道内径[M(P25,P75),mm] | 28(26,30) | 34(30,38) | -16.365 | <0.001 |
| 肺动脉内径[M(P25,P75),mm] | 24(23,26) | 30(26,33) | -17.064 | <0.001 |
表2 匹配后CPHD组与COPD组患者基线资料比较
Table 2 Comparison of baseline data between CPHD group and COPD group after matching
| 项目 | COPD组(n=469) | CPHD组(n=469) | Z(χ2)值 | P值 |
|---|---|---|---|---|
| 年龄[例(%)] | <0.001a | >0.999 | ||
| 20~39岁 | 2(0.4) | 2(0.4) | ||
| 40~59岁 | 69(14.7) | 69(14.7) | ||
| 60~79岁 | 281(59.9) | 281(59.9) | ||
| 80~99岁 | 117(25.0) | 117(25.0) | ||
| 饮酒[例(%)] | <0.001a | >0.999 | ||
| 无 | 401(85.5) | 401(85.5) | ||
| 有 | 68(14.5) | 68(14.5) | ||
| 心功能[例(%)] | 150.182a | <0.001 | ||
| 2级以下 | 423(90.2) | 255(54.4) | ||
| 3~4级 | 46(9.8) | 214(45.6) | ||
| HUA[例(%)] | 73.246a | <0.001 | ||
| 无 | 431(91.9) | 328(69.9) | ||
| 有 | 38(8.1) | 141(30.1) | ||
| 支气管哮喘[例(%)] | 22.602a | <0.001 | ||
| 无 | 332(70.8) | 393(83.8) | ||
| 有 | 137(29.2) | 76(16.2) | ||
| 淋巴细胞百分比[M(P25,P75),%] | 22.0(13.8,29.9) | 16.6(10.6,22.8) | -6.802 | <0.001 |
| 右心房内径[M(P25,P75),mm] | 33(32,35) | 42(36,46) | -18.863 | <0.001 |
| 右心室内径[M(P25,P75),mm] | 19(18,20) | 24(20,27) | -17.177 | <0.001 |
| 左心室舒张末期内径[M(P25,P75),mm] | 47(45,49) | 47(43,50) | -3.349 | <0.001 |
| 右心室流出道内径[M(P25,P75),mm] | 28(26,30) | 34(30,38) | -16.365 | <0.001 |
| 肺动脉内径[M(P25,P75),mm] | 24(23,26) | 30(26,33) | -17.064 | <0.001 |
| 变量 | 赋值 |
|---|---|
| CPHD | 否=0,是=1 |
| HUA | 否=0,是=1 |
| SUA四分位数分层 | Q1=0,Q2=1,Q3=2,Q4=3 |
| 心功能分级 | 2级以下=0,3~4级=1 |
| 支气管哮喘 | 无=0,有=1 |
| 右心房内径 | 实测值 |
| 右心室内径 | 实测值 |
| 左心室舒张末期内径 | 实测值 |
| 右心室流出道内径 | 实测值 |
| 肺动脉内径 | 实测值 |
表3 多因素Logistic回归分析变量赋值
Table 3 Multivariate Logistic regression analysis of variable assignment
| 变量 | 赋值 |
|---|---|
| CPHD | 否=0,是=1 |
| HUA | 否=0,是=1 |
| SUA四分位数分层 | Q1=0,Q2=1,Q3=2,Q4=3 |
| 心功能分级 | 2级以下=0,3~4级=1 |
| 支气管哮喘 | 无=0,有=1 |
| 右心房内径 | 实测值 |
| 右心室内径 | 实测值 |
| 左心室舒张末期内径 | 实测值 |
| 右心室流出道内径 | 实测值 |
| 肺动脉内径 | 实测值 |
| 变量 | B | SE | Wald χ2值 | OR(95%CI) | P值 |
|---|---|---|---|---|---|
| HUA | 1.228 | 0.269 | 20.808 | 3.414(2.014~5.786) | <0.001 |
| 心功能3~4级 | 1.400 | 0.239 | 34.467 | 4.056(2.542~6.474) | <0.001 |
| 支气管哮喘 | -0.618 | 0.234 | 6.967 | 0.539(0.340~0.853) | 0.008 |
| 淋巴细胞百分比 | -0.016 | 0.009 | 3.143 | 0.984(0.966~1.002) | 0.076 |
| 右心房内径 | 0.154 | 0.031 | 24.246 | 1.167(1.097~1.240) | <0.001 |
| 右心室内径 | 0.265 | 0.064 | 17.018 | 1.304(1.149~1.479) | <0.001 |
| 左心室舒张末期 | -0.098 | 0.023 | 17.632 | 0.907(0.866~0.949) | <0.001 |
| 右心室流出道内径 | -0.011 | 0.049 | 0.050 | 0.989(0.898~1.089) | 0.824 |
| 肺动脉内径 | 0.132 | 0.030 | 19.316 | 1.141(1.076~1.211) | <0.001 |
表4 COPD患者发生CPHD影响因素的多因素Logistic回归分析结果
Table 4 Multivariate Logistic regression analysis of CPHD in COPD patients
| 变量 | B | SE | Wald χ2值 | OR(95%CI) | P值 |
|---|---|---|---|---|---|
| HUA | 1.228 | 0.269 | 20.808 | 3.414(2.014~5.786) | <0.001 |
| 心功能3~4级 | 1.400 | 0.239 | 34.467 | 4.056(2.542~6.474) | <0.001 |
| 支气管哮喘 | -0.618 | 0.234 | 6.967 | 0.539(0.340~0.853) | 0.008 |
| 淋巴细胞百分比 | -0.016 | 0.009 | 3.143 | 0.984(0.966~1.002) | 0.076 |
| 右心房内径 | 0.154 | 0.031 | 24.246 | 1.167(1.097~1.240) | <0.001 |
| 右心室内径 | 0.265 | 0.064 | 17.018 | 1.304(1.149~1.479) | <0.001 |
| 左心室舒张末期 | -0.098 | 0.023 | 17.632 | 0.907(0.866~0.949) | <0.001 |
| 右心室流出道内径 | -0.011 | 0.049 | 0.050 | 0.989(0.898~1.089) | 0.824 |
| 肺动脉内径 | 0.132 | 0.030 | 19.316 | 1.141(1.076~1.211) | <0.001 |
| 项目 | COPD组(n=469) | CPHD组(n=469) | χ2值 | P值 |
|---|---|---|---|---|
| 分层 | 36.328 | <0.001 | ||
| Q1 | 125(26.7) | 102(21.7) | ||
| Q2 | 131(27.9) | 106(22.6) | ||
| Q3 | 130(27.7) | 97(20.7) | ||
| Q4 | 83(17.7) | 164(35.0) |
表5 匹配后CPHD组与COPD组患者SUA分层情况比较
Table 5 Comparison of SUA stratification between CPHD group and COPD group after matching
| 项目 | COPD组(n=469) | CPHD组(n=469) | χ2值 | P值 |
|---|---|---|---|---|
| 分层 | 36.328 | <0.001 | ||
| Q1 | 125(26.7) | 102(21.7) | ||
| Q2 | 131(27.9) | 106(22.6) | ||
| Q3 | 130(27.7) | 97(20.7) | ||
| Q4 | 83(17.7) | 164(35.0) |
| 变量 | B | SE | Wald χ2值 | OR(95%CI) | P值 |
|---|---|---|---|---|---|
| SUA分层(以Q1为参照) | |||||
| Q2 | -0.008 | 0.187 | 0.002 | 0.992(0.688~1.430) | 0.964 |
| Q3 | -0.089 | 0.189 | 0.224 | 0.914(0.631~1.325) | 0.636 |
| Q4 | 0.884 | 0.190 | 21.756 | 2.421(1.670~3.511) | <0.001 |
表6 SUA分层对患有CPHD影响的多因素Logistic回归分析结果
Table 6 Multivariate Logistic regression analysis of the effect of uric acid stratification on patients with CPHD
| 变量 | B | SE | Wald χ2值 | OR(95%CI) | P值 |
|---|---|---|---|---|---|
| SUA分层(以Q1为参照) | |||||
| Q2 | -0.008 | 0.187 | 0.002 | 0.992(0.688~1.430) | 0.964 |
| Q3 | -0.089 | 0.189 | 0.224 | 0.914(0.631~1.325) | 0.636 |
| Q4 | 0.884 | 0.190 | 21.756 | 2.421(1.670~3.511) | <0.001 |
| [1] |
|
| [2] |
滕长波. 老年人慢性肺源性心脏病发病危险因素分析[J]. 中西医结合心血管病电子杂志,2019,7(7):80,82. DOI:10.16282/j.cnki.cn11-9336/r.2019.07.055.
|
| [3] |
|
| [4] |
中华医学会呼吸病学分会慢性阻塞性肺疾病学组,中国医师协会呼吸医师分会慢性阻塞性肺疾病工作委员会. 慢性阻塞性肺疾病诊治指南(2021年修订版)[J]. 中华结核和呼吸杂志,2021,44(3):170-205. DOI:10.3760/cma.j.cn112147-20210109-00031.
|
| [5] |
中华医学会,中华医学会杂志社,中华医学会全科医学分会,等. 慢性肺源性心脏病基层诊疗指南(2018年)[J]. 中华全科医师杂志,2018,17(12):959-965. DOI:10.3760/cma.j.issn.1671-7368.2018.12.002.
|
| [6] |
World Health Organization. Guidelines for controlling and monitoring the tobacco epidemic[M].World Health Organization,Switzerland:1998.
|
| [7] |
中华医学会,中华医学会杂志社,中华医学会消化病学分会,等. 酒精性肝病基层诊疗指南(实践版·2019)[J]. 中华全科医师杂志,2020,19(11):997-1001. DOI:10.3760/cma.j.cn114798-20200812-00899.
|
| [8] |
中华医学会心血管病学分会心力衰竭学组,中国医师协会心力衰竭专业委员会,中华心血管病杂志编辑委员会. 中国心力衰竭诊断和治疗指南2018[J]. 中华心血管病杂志,2018,46(10):760-789. DOI:10.3760/cma.j.issn.0253-3758.2018.10.004.
|
| [9] |
World Health Organization. ICD-11 2022 release[EB/OL]. [2023-09-13].
|
| [10] |
|
| [11] |
方宁远,吕力为,吕晓希,等. 中国高尿酸血症相关疾病诊疗多学科专家共识(2023年版)[J]. 中国实用内科杂志,2023,43(6):461-480. DOI:10.19538/j.nk2023060106.
|
| [12] |
|
| [13] |
李赵进,冯爽,赵根明,等. 常见倾向性评分匹配方法在真实世界研究中的应用[J]. 中国卫生统计,2023,40(2):307-311.
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [1] | 王婷婷, 唐勇, 张文轲, 李志刚. 高尿酸血症运动干预的研究进展[J]. 中国全科医学, 2025, 28(30): 3841-3846. |
| [2] | 徐百川, 王艳, 张彭, 李艺婷, 刘飞来, 谢洋. 慢性阻塞性肺疾病共病肺癌筛查工具分析[J]. 中国全科医学, 2025, 28(30): 3847-3852. |
| [3] | 周鹏龙, 苌静, 丁素英, 陈静锋, 王涛, 李晨阳. 脂肪-肌肉比的年龄分层差异与高尿酸血症的相关性研究[J]. 中国全科医学, 2025, 28(27): 3375-3384. |
| [4] | 周倩, 吴晓敏, 王宝华, 严若菡, 蔚苗, 吴静. 胃癌发生风险的列线图预测模型研究[J]. 中国全科医学, 2025, 28(23): 2870-2877. |
| [5] | 张云静, 孙玥, 苏鹏, 赵永波, 马冬. 中青年急性Stanford A型主动脉夹层患者杂交手术与孙氏手术短期预后比较研究[J]. 中国全科医学, 2025, 28(21): 2618-2624. |
| [6] | 方莹莹, 林伟权, 孙敏英, 利耀辉, 刘览, 杨韵鸥, 陈嘉敏, 罗丽楹, 石磊, 刘慧. 屏幕时间对35岁及以上多重慢病患者睡眠质量的影响研究[J]. 中国全科医学, 2025, 28(20): 2501-2507. |
| [7] | 周韵哲, 苗竣翔, 韦杰桦, 陈立章, 王婷婷. 细胞周期蛋白D1和细胞周期蛋白E1基因多态性及其交互作用与先兆子痫的关联研究[J]. 中国全科医学, 2025, 28(17): 2142-2148. |
| [8] | 金锋, 黎旺玲, 谢飞. 基于"慢阻肺防治平台"的闭环管理案例研究[J]. 中国全科医学, 2025, 28(16): 2059-2064. |
| [9] | 陈典, 隆寰宇, 张丛溪, 褚岚和, 李姝润, 陈亚红. 2025年GOLD慢性阻塞性肺疾病诊断、治疗、管理及预防全球策略更新要点解读[J]. 中国全科医学, 2025, 28(16): 1937-1949. |
| [10] | 郦奇锋, 隆寰宇, 王泽茂, 封敏, 陈亚红, 胡征. 物联网技术在基层医疗卫生机构肺功能检查与管理中的应用[J]. 中国全科医学, 2025, 28(13): 1674-1675. |
| [11] | 宋荣维, 吴春香, 于杰, 路宇晴, 张锋英. 基于社区居民的保留比率的肺量计异常人群特征研究[J]. 中国全科医学, 2025, 28(10): 1185-1192. |
| [12] | 陈胜蓝, 郑永韬, 胡旺成, 倪作为, 夏冰, 叶春梅, 杜持新, 陈晓丹. 中小学生高度近视发生风险预测模型:基于巢式病例对照研究[J]. 中国全科医学, 2025, 28(09): 1115-1121. |
| [13] | 吴俊, 张玲, 顾东伟, 郑磊, 赵祝香, 赵子文. 单纯性支气管扩张症与支气管扩张症-慢性阻塞性肺疾病重叠综合征患者的病原菌对比研究[J]. 中国全科医学, 2025, 28(06): 729-736. |
| [14] | 张萍淑, 薛晶, 邢爱君, 王连辉, 马倩, 符永山, 元小冬. 急性后循环缺血性脑卒中患者睡眠状态变化与预后影响因素的研究[J]. 中国全科医学, 2025, 28(05): 548-553. |
| [15] | 袁淑娴, 林一凡, 赵艺璇, 魏怡, 鲁帅, 卫海燕. 黄体生成素/促卵泡生成素比值对快进展型中枢性性早熟的预测价值研究[J]. 中国全科医学, 2025, 28(03): 352-357. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||










