
中国全科医学 ›› 2024, Vol. 27 ›› Issue (07): 849-856.DOI: 10.12114/j.issn.1007-9572.2023.0413
所属专题: 健康公平性最新文章合辑
高点1, 史卢少博1, 林锦慧1, 王兴民2, 王冬1,*( )
)
收稿日期:2023-06-14
修回日期:2023-09-11
出版日期:2024-03-05
发布日期:2023-12-19
通讯作者:
王冬
基金资助:
GAO Dian1, SHI Lushaobo1, LIN Jinhui1, WANG Xingmin2, WANG Dong1,*()
Received:2023-06-14
Revised:2023-09-11
Published:2024-03-05
Online:2023-12-19
Contact:
WANG Dong
摘要: 背景 "强基层"是我国医改重心之一,研究我国农村医疗卫生资源配置的效率及公平性对推动基层医疗卫生服务有序发展具有重要意义,但目前罕有基于数据包络分析-地理信息系统(DEA-GIS)方法兼具公平和效率研究的相关文献。 目的 分析2020年我国29个省份农村医疗卫生资源配置的效率及公平性,为优化我国农村医疗卫生资源配置和完善乡村医疗卫生服务体系提供参考。 方法 本研究数据来源于《中华人民共和国行政区划统计表》《2021中国卫生健康统计年鉴》。综合现有文献研究、数据可得性及征得专家咨询意见,选取我国29个省份(不含北京市、上海市和港澳台地区)的乡镇卫生院和村卫生室作为研究对象,以乡镇卫生院和村卫生室机构数(以下简称卫生机构数)、乡镇卫生院床位数(以下简称床位数)、乡镇卫生院和村卫生室卫生技术人员数(以下简称卫生技术人员数)作为投入指标;乡镇卫生院和村卫生室诊疗人次数(以下简称诊疗数)、乡镇卫生院入院数(以下简称入院数)作为产出指标。运用DEA模型评估我国农村医疗卫生资源配置效率,利用卫生资源集聚度和GIS技术将农村医疗卫生资源配置情况进行空间制图,分析其公平性。 结果 2020年我国农村医疗卫生资源有4个省份DEA有效、7个省份DEA弱有效、18个省无效。其中,DEA无效地区均存在不同程度的投入过剩现象,仅山东省和西藏自治区存在产出不足的问题。分区域分析结果显示,农村医疗卫生资源集中分布在东部地区,中部地区次之,西部地区集聚度最低。 结论 政府需重视提升农村医疗卫生资源配置的技术效率,通过优化投入产出结构、减少资源冗余,合理统筹东中西部的资源配置,对各地区精准施策促进公平和效率。
| 地区 | 投入指标 | 产出指标 | |||
|---|---|---|---|---|---|
| 机构数(个) | 床位数(张) | 卫生技术人员数(人) | 诊疗数(万人次) | 入院数(万人次) | |
| 天津市 | 2 334 | 3 783 | 11 867 | 1 201.52 | 1.38 |
| 河北省 | 62 179 | 70 002 | 165 126 | 16 360.72 | 105.20 |
| 山西省 | 28 110 | 30 551 | 72 467 | 3 421.04 | 28.33 |
| 内蒙古自治区 | 14 287 | 21 481 | 49 234 | 2 359.88 | 20.28 |
| 辽宁省 | 18 591 | 31 011 | 50 313 | 3 905.34 | 30.71 |
| 吉林省 | 10 398 | 16 303 | 39 968 | 2 287.78 | 9.29 |
| 黑龙江省 | 11 351 | 23 715 | 49 138 | 1 858.90 | 23.60 |
| 江苏省 | 16 019 | 76 886 | 163 144 | 15 915.88 | 184.82 |
| 浙江省 | 12 358 | 20 211 | 78 357 | 14 289.10 | 26.55 |
| 安徽省 | 17 066 | 69 196 | 123 342 | 14 095.91 | 107.03 |
| 福建省 | 18 010 | 32 944 | 69 094 | 7 794.63 | 57.54 |
| 江西省 | 29 029 | 58 462 | 106 141 | 10 517.92 | 164.27 |
| 山东省 | 55 037 | 96 943 | 238 804 | 25 464.92 | 219.43 |
| 河南省 | 59 023 | 122 162 | 248 963 | 29 568.47 | 293.58 |
| 湖北省 | 24 320 | 80 429 | 134 413 | 11 637.16 | 239.46 |
| 湖南省 | 40 252 | 107 330 | 162 242 | 10 398.38 | 370.08 |
| 广东省 | 27 054 | 64 286 | 128 046 | 16 203.08 | 171.80 |
| 广西壮族自治区 | 20 563 | 72 947 | 110 738 | 7 138.96 | 280.13 |
| 海南省 | 3 041 | 7 710 | 18 385 | 1 387.29 | 4.35 |
| 重庆市 | 10 631 | 43 662 | 53 817 | 4 660.20 | 165.92 |
| 四川省 | 58 485 | 134 980 | 191 946 | 18 473.52 | 425.60 |
| 贵州省 | 21 492 | 44 600 | 87 677 | 6 286.92 | 117.94 |
| 云南省 | 14 954 | 54 899 | 103 358 | 11 258.04 | 150.42 |
| 西藏自治区 | 5 956 | 3 703 | 19 336 | 635.51 | 1.07 |
| 陕西省 | 24 501 | 35 743 | 84 583 | 5 726.41 | 50.74 |
| 甘肃省 | 17 785 | 28 606 | 64 547 | 3 508.76 | 67.47 |
| 青海省 | 4 884 | 4 720 | 16 065 | 618.13 | 8.18 |
| 宁夏回族自治区 | 2 377 | 3 657 | 11 913 | 1 024.09 | 3.76 |
| 新疆维吾尔自治区 | 10 862 | 29 403 | 48 960 | 3 491.99 | 54.40 |
表1 2020年我国农村医疗卫生资源投入、产出现状
Table 1 Current status of inputs and outputs of rural medical and health resources in China in 2020
| 地区 | 投入指标 | 产出指标 | |||
|---|---|---|---|---|---|
| 机构数(个) | 床位数(张) | 卫生技术人员数(人) | 诊疗数(万人次) | 入院数(万人次) | |
| 天津市 | 2 334 | 3 783 | 11 867 | 1 201.52 | 1.38 |
| 河北省 | 62 179 | 70 002 | 165 126 | 16 360.72 | 105.20 |
| 山西省 | 28 110 | 30 551 | 72 467 | 3 421.04 | 28.33 |
| 内蒙古自治区 | 14 287 | 21 481 | 49 234 | 2 359.88 | 20.28 |
| 辽宁省 | 18 591 | 31 011 | 50 313 | 3 905.34 | 30.71 |
| 吉林省 | 10 398 | 16 303 | 39 968 | 2 287.78 | 9.29 |
| 黑龙江省 | 11 351 | 23 715 | 49 138 | 1 858.90 | 23.60 |
| 江苏省 | 16 019 | 76 886 | 163 144 | 15 915.88 | 184.82 |
| 浙江省 | 12 358 | 20 211 | 78 357 | 14 289.10 | 26.55 |
| 安徽省 | 17 066 | 69 196 | 123 342 | 14 095.91 | 107.03 |
| 福建省 | 18 010 | 32 944 | 69 094 | 7 794.63 | 57.54 |
| 江西省 | 29 029 | 58 462 | 106 141 | 10 517.92 | 164.27 |
| 山东省 | 55 037 | 96 943 | 238 804 | 25 464.92 | 219.43 |
| 河南省 | 59 023 | 122 162 | 248 963 | 29 568.47 | 293.58 |
| 湖北省 | 24 320 | 80 429 | 134 413 | 11 637.16 | 239.46 |
| 湖南省 | 40 252 | 107 330 | 162 242 | 10 398.38 | 370.08 |
| 广东省 | 27 054 | 64 286 | 128 046 | 16 203.08 | 171.80 |
| 广西壮族自治区 | 20 563 | 72 947 | 110 738 | 7 138.96 | 280.13 |
| 海南省 | 3 041 | 7 710 | 18 385 | 1 387.29 | 4.35 |
| 重庆市 | 10 631 | 43 662 | 53 817 | 4 660.20 | 165.92 |
| 四川省 | 58 485 | 134 980 | 191 946 | 18 473.52 | 425.60 |
| 贵州省 | 21 492 | 44 600 | 87 677 | 6 286.92 | 117.94 |
| 云南省 | 14 954 | 54 899 | 103 358 | 11 258.04 | 150.42 |
| 西藏自治区 | 5 956 | 3 703 | 19 336 | 635.51 | 1.07 |
| 陕西省 | 24 501 | 35 743 | 84 583 | 5 726.41 | 50.74 |
| 甘肃省 | 17 785 | 28 606 | 64 547 | 3 508.76 | 67.47 |
| 青海省 | 4 884 | 4 720 | 16 065 | 618.13 | 8.18 |
| 宁夏回族自治区 | 2 377 | 3 657 | 11 913 | 1 024.09 | 3.76 |
| 新疆维吾尔自治区 | 10 862 | 29 403 | 48 960 | 3 491.99 | 54.40 |
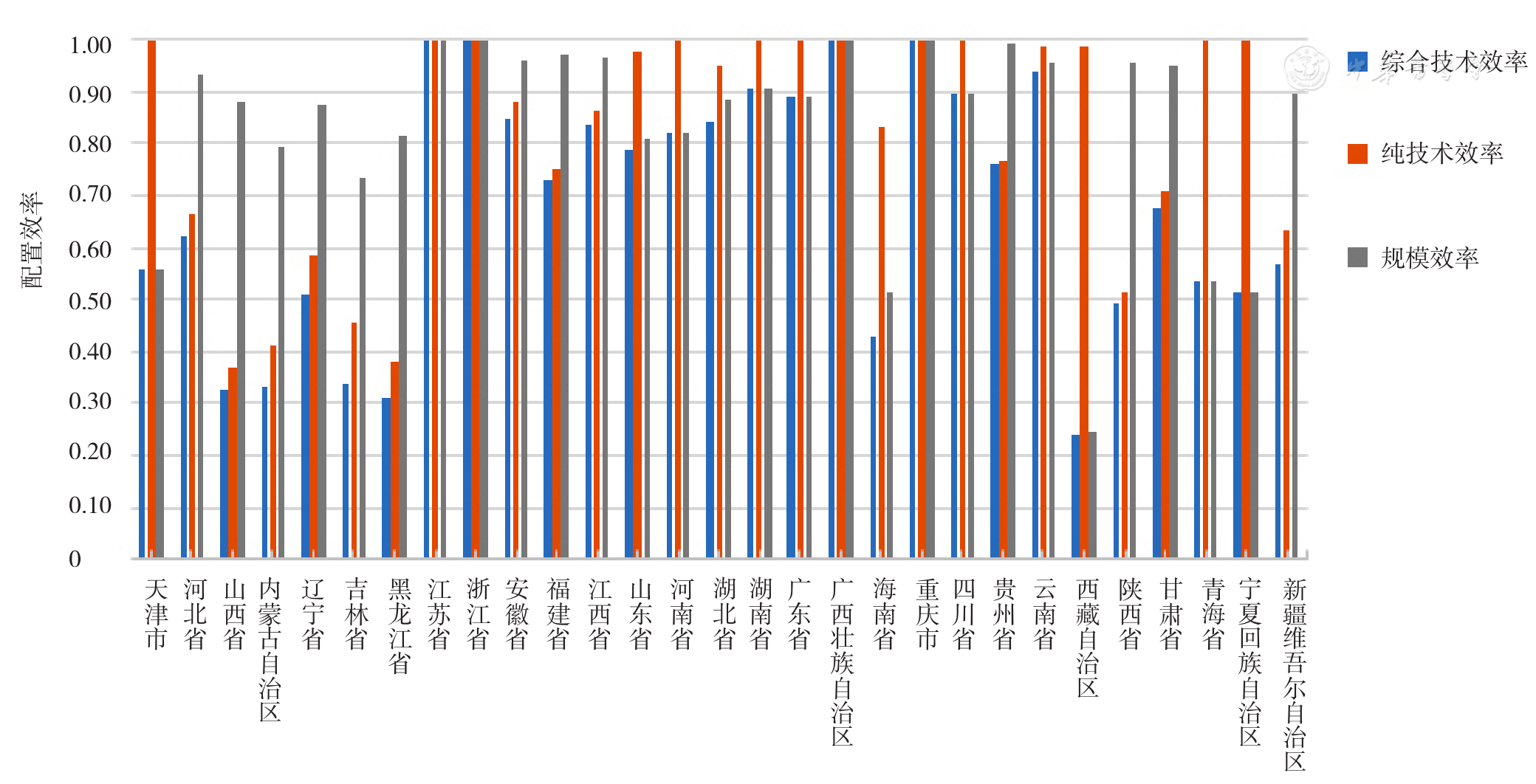
图1 2020年我国农村医疗卫生资源配置效率分布图
Figure 1 Distribution of rural medical and health resources allocation efficiency in China in 2020
| 地区 | 综合技术效率 | 纯技术效率 | 规模效率 | 规模效应 | DEA有效性 |
|---|---|---|---|---|---|
| 天津市 | 0.56 | 1.00 | 0.56 | irs | 弱有效 |
| 河北省 | 0.63 | 0.67 | 0.94 | drs | 无效 |
| 山西省 | 0.33 | 0.37 | 0.88 | irs | 无效 |
| 内蒙古自治区 | 0.33 | 0.42 | 0.80 | irs | 无效 |
| 辽宁省 | 0.51 | 0.58 | 0.87 | irs | 无效 |
| 吉林省 | 0.34 | 0.46 | 0.74 | irs | 无效 |
| 黑龙江省 | 0.31 | 0.38 | 0.82 | irs | 无效 |
| 江苏省 | 1.00 | 1.00 | 1.00 | - | 有效 |
| 浙江省 | 1.00 | 1.00 | 1.00 | - | 有效 |
| 安徽省 | 0.85 | 0.88 | 0.96 | drs | 无效 |
| 福建省 | 0.73 | 0.75 | 0.97 | irs | 无效 |
| 江西省 | 0.84 | 0.87 | 0.97 | drs | 无效 |
| 山东省 | 0.79 | 0.98 | 0.81 | drs | 无效 |
| 河南省 | 0.82 | 1.00 | 0.82 | drs | 弱有效 |
| 湖北省 | 0.84 | 0.95 | 0.89 | drs | 无效 |
| 湖南省 | 0.91 | 1.00 | 0.91 | drs | 弱有效 |
| 广东省 | 0.89 | 1.00 | 0.89 | drs | 弱有效 |
| 广西壮族自治区 | 1.00 | 1.00 | 1.00 | - | 有效 |
| 海南省 | 0.43 | 0.83 | 0.52 | irs | 无效 |
| 重庆市 | 1.00 | 1.00 | 1.00 | - | 有效 |
| 四川省 | 0.89 | 1.00 | 0.89 | drs | 弱有效 |
| 贵州省 | 0.76 | 0.77 | 0.99 | irs | 无效 |
| 云南省 | 0.94 | 0.99 | 0.95 | drs | 无效 |
| 西藏自治区 | 0.24 | 0.99 | 0.25 | irs | 无效 |
| 陕西省 | 0.49 | 0.51 | 0.96 | irs | 无效 |
| 甘肃省 | 0.68 | 0.71 | 0.95 | irs | 无效 |
| 青海省 | 0.54 | 1.00 | 0.54 | irs | 弱有效 |
| 宁夏回族自治区 | 0.52 | 1.00 | 0.52 | irs | 弱有效 |
| 新疆维吾尔自治区 | 0.57 | 0.63 | 0.90 | irs | 无效 |
| 均值 | 0.68 | 0.82 | 0.84 |
表2 2020年我国农村医疗卫生资源配置效率分析
Table 2 Analysis of the allocation efficiency of rural medical and health resources in China in 2020
| 地区 | 综合技术效率 | 纯技术效率 | 规模效率 | 规模效应 | DEA有效性 |
|---|---|---|---|---|---|
| 天津市 | 0.56 | 1.00 | 0.56 | irs | 弱有效 |
| 河北省 | 0.63 | 0.67 | 0.94 | drs | 无效 |
| 山西省 | 0.33 | 0.37 | 0.88 | irs | 无效 |
| 内蒙古自治区 | 0.33 | 0.42 | 0.80 | irs | 无效 |
| 辽宁省 | 0.51 | 0.58 | 0.87 | irs | 无效 |
| 吉林省 | 0.34 | 0.46 | 0.74 | irs | 无效 |
| 黑龙江省 | 0.31 | 0.38 | 0.82 | irs | 无效 |
| 江苏省 | 1.00 | 1.00 | 1.00 | - | 有效 |
| 浙江省 | 1.00 | 1.00 | 1.00 | - | 有效 |
| 安徽省 | 0.85 | 0.88 | 0.96 | drs | 无效 |
| 福建省 | 0.73 | 0.75 | 0.97 | irs | 无效 |
| 江西省 | 0.84 | 0.87 | 0.97 | drs | 无效 |
| 山东省 | 0.79 | 0.98 | 0.81 | drs | 无效 |
| 河南省 | 0.82 | 1.00 | 0.82 | drs | 弱有效 |
| 湖北省 | 0.84 | 0.95 | 0.89 | drs | 无效 |
| 湖南省 | 0.91 | 1.00 | 0.91 | drs | 弱有效 |
| 广东省 | 0.89 | 1.00 | 0.89 | drs | 弱有效 |
| 广西壮族自治区 | 1.00 | 1.00 | 1.00 | - | 有效 |
| 海南省 | 0.43 | 0.83 | 0.52 | irs | 无效 |
| 重庆市 | 1.00 | 1.00 | 1.00 | - | 有效 |
| 四川省 | 0.89 | 1.00 | 0.89 | drs | 弱有效 |
| 贵州省 | 0.76 | 0.77 | 0.99 | irs | 无效 |
| 云南省 | 0.94 | 0.99 | 0.95 | drs | 无效 |
| 西藏自治区 | 0.24 | 0.99 | 0.25 | irs | 无效 |
| 陕西省 | 0.49 | 0.51 | 0.96 | irs | 无效 |
| 甘肃省 | 0.68 | 0.71 | 0.95 | irs | 无效 |
| 青海省 | 0.54 | 1.00 | 0.54 | irs | 弱有效 |
| 宁夏回族自治区 | 0.52 | 1.00 | 0.52 | irs | 弱有效 |
| 新疆维吾尔自治区 | 0.57 | 0.63 | 0.90 | irs | 无效 |
| 均值 | 0.68 | 0.82 | 0.84 |
| 地区 | 投入指标 | 产出指标 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| S-(X1) | 理想值 | S-(X2) | 理想值 | S-(X3) | 理想值 | S+(Y1) | 理想值 | S+(Y2) | 理想值 | |
| 河北省 | 39 150.99 | 23 028.02 | 24 657.31 | 45 344.69 | 54 929.25 | 110 196.75 | 0 | 11 360.72 | 0 | 105.20 |
| 山西省 | 21 215.77 | 1 894.24 | 11 184.62 | 11 366.39 | 41 505.93 | 21 961.08 | 0 | 1 421.04 | 0 | 28.34 |
| 内蒙古自治区 | 11 456.49 | 1 830.51 | 11 575.97 | 1 905.03 | 21 823.87 | 21 410.13 | 0 | 1 359.88 | 0 | 20.28 |
| 辽宁省 | 11323.02 | 1 267.98 | 11 403.46 | 11 607.54 | 21 984.16 | 21 328.84 | 0 | 1 905.34 | 0 | 30.71 |
| 吉林省 | 1 023.86 | 1 374.14 | 1 846.72 | 1 456.28 | 21 683.89 | 11 284.11 | 0 | 1 287.78 | 0 | 9.29 |
| 黑龙江省 | 1 719.30 | 1 631.70 | 11 674.99 | 1 040.01 | 31 406.90 | 11 731.10 | 0 | 1 858.90 | 0 | 23.60 |
| 安徽省 | 1 029.36 | 11 036.64 | 21 628.34 | 41 567.66 | 11 666.90 | 101 675.10 | 0 | 11 095.91 | 0 | 107.03 |
| 福建省 | 1 070.89 | 1 939.11 | 11 098.73 | 21 845.27 | 11 018.03 | 51 075.97 | 0 | 1 794.63 | 0 | 57.54 |
| 江西省 | 11 532.67 | 11 496.33 | 1 896.54 | 51 565.46 | 11 336.60 | 91 804.40 | 0 | 11 517.92 | 0 | 164.27 |
| 山东省 | 1 546.73 | 41 490.27 | 1 161.79 | 91 781.21 | 31 660.34 | 201 143.66 | 0 | 21 464.92 | 2.44 | 221.87 |
| 湖北省 | 1 223.88 | 21 096.12 | 1 047.50 | 71 381.50 | 1 764.19 | 121 648.82 | 0 | 11 637.16 | 0 | 239.46 |
| 海南省 | 506.95 | 1 534.05 | 1 882.21 | 1 827.79 | 1 573.75 | 11 811.25 | 0 | 1 387.30 | 0 | 4.35 |
| 贵州省 | 11 433.93 | 11 058.07 | 11 457.60 | 31 142.40 | 31 426.55 | 51 250.45 | 0 | 1 286.92 | 0 | 117.94 |
| 云南省 | 203.44 | 11 750.56 | 1 793.77 | 51 105.23 | 1 406.09 | 101 951.91 | 0 | 11 258.04 | 0 | 150.42 |
| 西藏自治区 | 1 579.00 | 1 377.00 | 46.00 | 1 657.00 | 1 423.00 | 11 913.00 | 388.58 | 1 024.09 | 2.69 | 3.76 |
| 陕西省 | 11 209.04 | 1 291.96 | 11 368.51 | 11 374.49 | 41 205.25 | 41 377.75 | 0 | 1 726.41 | 0 | 50.74 |
| 甘肃省 | 11 434.79 | 1 350.21 | 1 327.00 | 21 279.00 | 31 156.65 | 31 390.36 | 0 | 1 508.76 | 0 | 67.47 |
| 新疆维吾尔自治区 | 1 034.81 | 1 827.19 | 11 803.68 | 11 599.32 | 11 950.88 | 31 009.12 | 0 | 1 491.99 | 0 | 54.40 |
表3 非DEA有效省份农村医疗卫生资源配置效率的松弛变量、理想值
Table 3 Relaxation variables and ideal values of the allocation efficiency of rural medical and health resources in non-DEA efficient provinces
| 地区 | 投入指标 | 产出指标 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| S-(X1) | 理想值 | S-(X2) | 理想值 | S-(X3) | 理想值 | S+(Y1) | 理想值 | S+(Y2) | 理想值 | |
| 河北省 | 39 150.99 | 23 028.02 | 24 657.31 | 45 344.69 | 54 929.25 | 110 196.75 | 0 | 11 360.72 | 0 | 105.20 |
| 山西省 | 21 215.77 | 1 894.24 | 11 184.62 | 11 366.39 | 41 505.93 | 21 961.08 | 0 | 1 421.04 | 0 | 28.34 |
| 内蒙古自治区 | 11 456.49 | 1 830.51 | 11 575.97 | 1 905.03 | 21 823.87 | 21 410.13 | 0 | 1 359.88 | 0 | 20.28 |
| 辽宁省 | 11323.02 | 1 267.98 | 11 403.46 | 11 607.54 | 21 984.16 | 21 328.84 | 0 | 1 905.34 | 0 | 30.71 |
| 吉林省 | 1 023.86 | 1 374.14 | 1 846.72 | 1 456.28 | 21 683.89 | 11 284.11 | 0 | 1 287.78 | 0 | 9.29 |
| 黑龙江省 | 1 719.30 | 1 631.70 | 11 674.99 | 1 040.01 | 31 406.90 | 11 731.10 | 0 | 1 858.90 | 0 | 23.60 |
| 安徽省 | 1 029.36 | 11 036.64 | 21 628.34 | 41 567.66 | 11 666.90 | 101 675.10 | 0 | 11 095.91 | 0 | 107.03 |
| 福建省 | 1 070.89 | 1 939.11 | 11 098.73 | 21 845.27 | 11 018.03 | 51 075.97 | 0 | 1 794.63 | 0 | 57.54 |
| 江西省 | 11 532.67 | 11 496.33 | 1 896.54 | 51 565.46 | 11 336.60 | 91 804.40 | 0 | 11 517.92 | 0 | 164.27 |
| 山东省 | 1 546.73 | 41 490.27 | 1 161.79 | 91 781.21 | 31 660.34 | 201 143.66 | 0 | 21 464.92 | 2.44 | 221.87 |
| 湖北省 | 1 223.88 | 21 096.12 | 1 047.50 | 71 381.50 | 1 764.19 | 121 648.82 | 0 | 11 637.16 | 0 | 239.46 |
| 海南省 | 506.95 | 1 534.05 | 1 882.21 | 1 827.79 | 1 573.75 | 11 811.25 | 0 | 1 387.30 | 0 | 4.35 |
| 贵州省 | 11 433.93 | 11 058.07 | 11 457.60 | 31 142.40 | 31 426.55 | 51 250.45 | 0 | 1 286.92 | 0 | 117.94 |
| 云南省 | 203.44 | 11 750.56 | 1 793.77 | 51 105.23 | 1 406.09 | 101 951.91 | 0 | 11 258.04 | 0 | 150.42 |
| 西藏自治区 | 1 579.00 | 1 377.00 | 46.00 | 1 657.00 | 1 423.00 | 11 913.00 | 388.58 | 1 024.09 | 2.69 | 3.76 |
| 陕西省 | 11 209.04 | 1 291.96 | 11 368.51 | 11 374.49 | 41 205.25 | 41 377.75 | 0 | 1 726.41 | 0 | 50.74 |
| 甘肃省 | 11 434.79 | 1 350.21 | 1 327.00 | 21 279.00 | 31 156.65 | 31 390.36 | 0 | 1 508.76 | 0 | 67.47 |
| 新疆维吾尔自治区 | 1 034.81 | 1 827.19 | 11 803.68 | 11 599.32 | 11 950.88 | 31 009.12 | 0 | 1 491.99 | 0 | 54.40 |
| 地区 | 变量 | 机构数(个) | 床位数(张) | 卫生技术人员数(人) | 诊疗数(万人次) | 入院数(万人) |
|---|---|---|---|---|---|---|
| 河北省 | 实际值 | 62 179 | 70 002 | 1 65 126 | 11 360.72 | 105.20 |
| 目标值 | 21 028.02 | 41 344.69 | 111 196.75 | 11 360.72 | 105.20 | |
| 改进比例(%) | -0.63 | -0.35 | -0.33 | 0 | 0 | |
| 山西省 | 实际值 | 28 110 | 30 551 | 72 467 | 1 421.04 | 28.34 |
| 目标值 | 1 894.24 | 11 366.39 | 21 961.08 | 1 421.04 | 28.34 | |
| 改进比例(%) | -0.83 | -0.63 | -0.63 | 0 | 0 | |
| 内蒙古自治区 | 实际值 | 14 287 | 21 481 | 49 234 | 1 359.88 | 20.28 |
| 目标值 | 1 830.51 | 1 905.03 | 21 410.13 | 1 359.88 | 20.28 | |
| 改进比例(%) | -0.73 | -0.59 | -0.59 | 0 | 0 | |
| 辽宁省 | 实际值 | 18 591 | 31 011 | 50 313 | 1 905.34 | 30.71 |
| 目标值 | 1 267.98 | 11 607.54 | 21 328.84 | 1 905.34 | 30.71 | |
| 改进比例(%) | -0.72 | -0.59 | -0.42 | 0 | 0 | |
| 吉林省 | 实际值 | 10 398 | 16 303 | 39 968 | 1 287.78 | 9.29 |
| 目标值 | 1 374.14 | 1 456.28 | 11 284.11 | 1 287.78 | 9.29 | |
| 改进比例(%) | -0.68 | -0.60 | -0.54 | 0 | 0 | |
| 黑龙江省 | 实际值 | 11 351 | 23 715 | 49 138 | 1 858.90 | 23.60 |
| 目标值 | 1 631.70 | 1 040.01 | 11 731.10 | 1 858.90 | 23.60 | |
| 改进比例(%) | -0.68 | -0.62 | -0.62 | 0 | 0 | |
| 安徽省 | 实际值 | 17 066 | 69 196 | 123 342 | 11 095.91 | 107.03 |
| 目标值 | 11 036.64 | 41 567.66 | 101 675.10 | 11 095.91 | 107.03 | |
| 改进比例(%) | -0.12 | -0.34 | -0.12 | 0 | 0 | |
| 福建省 | 实际值 | 18 010 | 32 944 | 69 094 | 1 794.63 | 57.54 |
| 目标值 | 1 939.11 | 21 845.27 | 51 075.97 | 1 794.63 | 57.54 | |
| 改进比例(%) | -0.50 | -0.34 | -0.25 | 0 | 0 | |
| 江西省 | 实际值 | 29 029 | 58 462 | 106 141 | 11 517.92 | 164.27 |
| 目标值 | 11 496.33 | 51 565.46 | 91 804.40 | 11 517.92 | 164.27 | |
| 改进比例(%) | -0.36 | -0.14 | -0.14 | 0 | 0 | |
| 山东省 | 实际值 | 55 037 | 96 943 | 138 804 | 21 464.92 | 219.43 |
| 目标值 | 41 490.27 | 91 781.21 | 201 143.66 | 21 464.92 | 221.87 | |
| 改进比例(%) | -0.16 | -0.02 | -0.15 | 0 | 0.01 | |
| 湖北省 | 实际值 | 24 320 | 80 429 | 134 413 | 11 637.16 | 239.46 |
| 目标值 | 21 096.12 | 71 381.50 | 121 648.82 | 11 637.16 | 239.46 | |
| 改进比例(%) | -0.05 | -0.05 | -0.05 | 0 | 0 | |
| 海南省 | 实际值 | 3 041 | 7 710 | 18 385 | 1 387.30 | 4.35 |
| 目标值 | 1 534.05 | 1 827.79 | 11 811.25 | 1 387.30 | 4.35 | |
| 改进比例(%) | -0.17 | -0.37 | -0.25 | 0 | 0 | |
| 贵州省 | 实际值 | 21 492 | 44 600 | 87 677 | 1 286.92 | 117.94 |
| 目标值 | 11 058.07 | 31 142.4 | 51 250.45 | 1 286.92 | 117.94 | |
| 改进比例(%) | -0.53 | -0.23 | -0.38 | 0 | 0 | |
| 云南省 | 实际值 | 14 954 | 54 899 | 103 358 | 11 258.04 | 150.42 |
| 目标值 | 11 750.56 | 51 105.23 | 101 951.91 | 11 258.04 | 150.42 | |
| 改进比例(%) | -0.01 | -0.03 | -0.01 | 0 | 0 | |
| 西藏自治区 | 实际值 | 5 956 | 3 703 | 19 336 | 635.51 | 1.07 |
| 目标值 | 2 377 | 3 657 | 11 913 | 1 024.09 | 3.76 | |
| 改进比例(%) | -0.60 | -0.01 | -0.38 | 0.61 | 2.52 | |
| 陕西省 | 实际值 | 24 501 | 35 743 | 84 583 | 1 726.41 | 50.74 |
| 目标值 | 1 291.96 | 11 374.49 | 41 377.75 | 1 726.41 | 50.74 | |
| 改进比例(%) | -0.70 | -0.49 | -0.51 | 0 | 0 | |
| 甘肃省 | 实际值 | 17 785 | 28 606 | 64 547 | 1 508.76 | 67.47 |
| 目标值 | 1 350.21 | 20 279 | 31 390.36 | 1 508.76 | 67.47 | |
| 改进比例(%) | -0.64 | -0.29 | -0.48 | 0 | 0 | |
| 新疆维吾尔自治区 | 实际值 | 10 862 | 29 403 | 48 960 | 1 491.99 | 54.40 |
| 目标值 | 1 827.19 | 11 599.32 | 31 009.12 | 1 491.99 | 54.40 | |
| 改进比例(%) | -0.46 | -0.40 | -0.37 | 0 | 0 |
表4 非DEA有效省份农村医疗卫生资源投入与产出的实际值和目标值比较
Table 4 Comparison of actual and target values of input and output of rural medical and health resources in non-DEA effective provinces
| 地区 | 变量 | 机构数(个) | 床位数(张) | 卫生技术人员数(人) | 诊疗数(万人次) | 入院数(万人) |
|---|---|---|---|---|---|---|
| 河北省 | 实际值 | 62 179 | 70 002 | 1 65 126 | 11 360.72 | 105.20 |
| 目标值 | 21 028.02 | 41 344.69 | 111 196.75 | 11 360.72 | 105.20 | |
| 改进比例(%) | -0.63 | -0.35 | -0.33 | 0 | 0 | |
| 山西省 | 实际值 | 28 110 | 30 551 | 72 467 | 1 421.04 | 28.34 |
| 目标值 | 1 894.24 | 11 366.39 | 21 961.08 | 1 421.04 | 28.34 | |
| 改进比例(%) | -0.83 | -0.63 | -0.63 | 0 | 0 | |
| 内蒙古自治区 | 实际值 | 14 287 | 21 481 | 49 234 | 1 359.88 | 20.28 |
| 目标值 | 1 830.51 | 1 905.03 | 21 410.13 | 1 359.88 | 20.28 | |
| 改进比例(%) | -0.73 | -0.59 | -0.59 | 0 | 0 | |
| 辽宁省 | 实际值 | 18 591 | 31 011 | 50 313 | 1 905.34 | 30.71 |
| 目标值 | 1 267.98 | 11 607.54 | 21 328.84 | 1 905.34 | 30.71 | |
| 改进比例(%) | -0.72 | -0.59 | -0.42 | 0 | 0 | |
| 吉林省 | 实际值 | 10 398 | 16 303 | 39 968 | 1 287.78 | 9.29 |
| 目标值 | 1 374.14 | 1 456.28 | 11 284.11 | 1 287.78 | 9.29 | |
| 改进比例(%) | -0.68 | -0.60 | -0.54 | 0 | 0 | |
| 黑龙江省 | 实际值 | 11 351 | 23 715 | 49 138 | 1 858.90 | 23.60 |
| 目标值 | 1 631.70 | 1 040.01 | 11 731.10 | 1 858.90 | 23.60 | |
| 改进比例(%) | -0.68 | -0.62 | -0.62 | 0 | 0 | |
| 安徽省 | 实际值 | 17 066 | 69 196 | 123 342 | 11 095.91 | 107.03 |
| 目标值 | 11 036.64 | 41 567.66 | 101 675.10 | 11 095.91 | 107.03 | |
| 改进比例(%) | -0.12 | -0.34 | -0.12 | 0 | 0 | |
| 福建省 | 实际值 | 18 010 | 32 944 | 69 094 | 1 794.63 | 57.54 |
| 目标值 | 1 939.11 | 21 845.27 | 51 075.97 | 1 794.63 | 57.54 | |
| 改进比例(%) | -0.50 | -0.34 | -0.25 | 0 | 0 | |
| 江西省 | 实际值 | 29 029 | 58 462 | 106 141 | 11 517.92 | 164.27 |
| 目标值 | 11 496.33 | 51 565.46 | 91 804.40 | 11 517.92 | 164.27 | |
| 改进比例(%) | -0.36 | -0.14 | -0.14 | 0 | 0 | |
| 山东省 | 实际值 | 55 037 | 96 943 | 138 804 | 21 464.92 | 219.43 |
| 目标值 | 41 490.27 | 91 781.21 | 201 143.66 | 21 464.92 | 221.87 | |
| 改进比例(%) | -0.16 | -0.02 | -0.15 | 0 | 0.01 | |
| 湖北省 | 实际值 | 24 320 | 80 429 | 134 413 | 11 637.16 | 239.46 |
| 目标值 | 21 096.12 | 71 381.50 | 121 648.82 | 11 637.16 | 239.46 | |
| 改进比例(%) | -0.05 | -0.05 | -0.05 | 0 | 0 | |
| 海南省 | 实际值 | 3 041 | 7 710 | 18 385 | 1 387.30 | 4.35 |
| 目标值 | 1 534.05 | 1 827.79 | 11 811.25 | 1 387.30 | 4.35 | |
| 改进比例(%) | -0.17 | -0.37 | -0.25 | 0 | 0 | |
| 贵州省 | 实际值 | 21 492 | 44 600 | 87 677 | 1 286.92 | 117.94 |
| 目标值 | 11 058.07 | 31 142.4 | 51 250.45 | 1 286.92 | 117.94 | |
| 改进比例(%) | -0.53 | -0.23 | -0.38 | 0 | 0 | |
| 云南省 | 实际值 | 14 954 | 54 899 | 103 358 | 11 258.04 | 150.42 |
| 目标值 | 11 750.56 | 51 105.23 | 101 951.91 | 11 258.04 | 150.42 | |
| 改进比例(%) | -0.01 | -0.03 | -0.01 | 0 | 0 | |
| 西藏自治区 | 实际值 | 5 956 | 3 703 | 19 336 | 635.51 | 1.07 |
| 目标值 | 2 377 | 3 657 | 11 913 | 1 024.09 | 3.76 | |
| 改进比例(%) | -0.60 | -0.01 | -0.38 | 0.61 | 2.52 | |
| 陕西省 | 实际值 | 24 501 | 35 743 | 84 583 | 1 726.41 | 50.74 |
| 目标值 | 1 291.96 | 11 374.49 | 41 377.75 | 1 726.41 | 50.74 | |
| 改进比例(%) | -0.70 | -0.49 | -0.51 | 0 | 0 | |
| 甘肃省 | 实际值 | 17 785 | 28 606 | 64 547 | 1 508.76 | 67.47 |
| 目标值 | 1 350.21 | 20 279 | 31 390.36 | 1 508.76 | 67.47 | |
| 改进比例(%) | -0.64 | -0.29 | -0.48 | 0 | 0 | |
| 新疆维吾尔自治区 | 实际值 | 10 862 | 29 403 | 48 960 | 1 491.99 | 54.40 |
| 目标值 | 1 827.19 | 11 599.32 | 31 009.12 | 1 491.99 | 54.40 | |
| 改进比例(%) | -0.46 | -0.40 | -0.37 | 0 | 0 |
| 地区 | 改进原因 | 改进参考集 |
|---|---|---|
| 河北省 | 投入过剩 | 浙江省、河南省、四川省 |
| 山西省 | 投入过剩 | 天津市、浙江省、重庆市、宁夏回族自治区 |
| 内蒙古自治区 | 投入过剩 | 天津市、浙江省、重庆市、宁夏回族自治区 |
| 辽宁省 | 投入过剩 | 天津市、浙江省、重庆市 |
| 吉林省 | 投入过剩 | 天津市、浙江省、重庆市 |
| 黑龙江省 | 投入过剩 | 天津市、浙江省、重庆市、宁夏回族自治区 |
| 安徽省 | 投入过剩 | 江苏省、浙江省、广东省、重庆市 |
| 福建省 | 投入过剩 | 天津市、浙江省、重庆市 |
| 江西省 | 投入过剩 | 浙江省、广西壮族自治区、重庆市、四川省 |
| 山东省 | 投入过剩,产出不足 | 浙江省、河南省 |
| 湖北省 | 投入过剩 | 江苏省、广东省、广西壮族自治区、重庆市、四川省 |
| 海南省 | 投入过剩 | 天津市、江苏省、重庆市 |
| 贵州省 | 投入过剩 | 浙江省、重庆市、宁夏回族自治区 |
| 云南省 | 投入过剩 | 江苏省、浙江省、广东省、重庆市 |
| 西藏自治区 | 投入过剩,产出不足 | 宁夏回族自治区 |
| 陕西省 | 投入过剩 | 浙江省、重庆市、宁夏回族自治区 |
| 甘肃省 | 投入过剩 | 浙江省、重庆市、宁夏回族自治区 |
| 新疆维吾尔自治区 | 投入过剩 | 天津市、浙江省、重庆市 |
表5 非DEA有效省份农村医疗卫生资源配置效率的改进原因和参考集
Table 5 Reasons for improvement and reference sets of rural medical and health resources allocation efficiency in non-DEA-effective provinces
| 地区 | 改进原因 | 改进参考集 |
|---|---|---|
| 河北省 | 投入过剩 | 浙江省、河南省、四川省 |
| 山西省 | 投入过剩 | 天津市、浙江省、重庆市、宁夏回族自治区 |
| 内蒙古自治区 | 投入过剩 | 天津市、浙江省、重庆市、宁夏回族自治区 |
| 辽宁省 | 投入过剩 | 天津市、浙江省、重庆市 |
| 吉林省 | 投入过剩 | 天津市、浙江省、重庆市 |
| 黑龙江省 | 投入过剩 | 天津市、浙江省、重庆市、宁夏回族自治区 |
| 安徽省 | 投入过剩 | 江苏省、浙江省、广东省、重庆市 |
| 福建省 | 投入过剩 | 天津市、浙江省、重庆市 |
| 江西省 | 投入过剩 | 浙江省、广西壮族自治区、重庆市、四川省 |
| 山东省 | 投入过剩,产出不足 | 浙江省、河南省 |
| 湖北省 | 投入过剩 | 江苏省、广东省、广西壮族自治区、重庆市、四川省 |
| 海南省 | 投入过剩 | 天津市、江苏省、重庆市 |
| 贵州省 | 投入过剩 | 浙江省、重庆市、宁夏回族自治区 |
| 云南省 | 投入过剩 | 江苏省、浙江省、广东省、重庆市 |
| 西藏自治区 | 投入过剩,产出不足 | 宁夏回族自治区 |
| 陕西省 | 投入过剩 | 浙江省、重庆市、宁夏回族自治区 |
| 甘肃省 | 投入过剩 | 浙江省、重庆市、宁夏回族自治区 |
| 新疆维吾尔自治区 | 投入过剩 | 天津市、浙江省、重庆市 |
| 地区 | 卫生机构数 | 床位数 | 卫生技术人员数 |
|---|---|---|---|
| 天津市 | 2.92 | 2.18 | 3.52 |
| 河北省 | 4.91 | 2.55 | 3.09 |
| 山西省 | 2.64 | 1.32 | 1.61 |
| 内蒙古自治区 | 0.18 | 0.13 | 0.15 |
| 辽宁省 | 1.86 | 1.43 | 1.19 |
| 吉林省 | 0.82 | 0.59 | 0.75 |
| 黑龙江省 | 0.37 | 0.36 | 0.38 |
| 江苏省 | 2.40 | 5.32 | 5.80 |
| 浙江省 | 1.85 | 1.40 | 2.79 |
| 安徽省 | 1.83 | 3.42 | 3.13 |
| 福建省 | 2.25 | 1.90 | 2.05 |
| 江西省 | 2.56 | 2.38 | 2.22 |
| 山东省 | 5.16 | 4.19 | 5.31 |
| 河南省 | 5.21 | 4.97 | 5.21 |
| 湖北省 | 1.92 | 2.93 | 2.52 |
| 湖南省 | 2.88 | 3.53 | 2.75 |
| 广东省 | 2.25 | 2.47 | 2.53 |
| 广西壮族自治区 | 1.29 | 2.10 | 1.64 |
| 海南省 | 1.34 | 1.57 | 1.92 |
| 重庆市 | 1.94 | 3.68 | 2.34 |
| 四川省 | 1.79 | 1.90 | 1.39 |
| 贵州省 | 1.79 | 1.71 | 1.73 |
| 云南省 | 0.58 | 0.97 | 0.94 |
| 西藏自治区 | 0.07 | 0.02 | 0.06 |
| 陕西省 | 1.75 | 1.18 | 1.43 |
| 甘肃省 | 0.62 | 0.46 | 0.53 |
| 青海省 | 0.10 | 0.05 | 0.08 |
| 宁夏回族自治区 | 0.54 | 0.38 | 0.64 |
| 新疆维吾尔自治区 | 0.10 | 0.12 | 0.10 |
表6 2020年我国农村医疗卫生资源投入指标的集聚度
Table 6 The health resource agglomeration degree of rural medical and health resource input indicators in China in 2020
| 地区 | 卫生机构数 | 床位数 | 卫生技术人员数 |
|---|---|---|---|
| 天津市 | 2.92 | 2.18 | 3.52 |
| 河北省 | 4.91 | 2.55 | 3.09 |
| 山西省 | 2.64 | 1.32 | 1.61 |
| 内蒙古自治区 | 0.18 | 0.13 | 0.15 |
| 辽宁省 | 1.86 | 1.43 | 1.19 |
| 吉林省 | 0.82 | 0.59 | 0.75 |
| 黑龙江省 | 0.37 | 0.36 | 0.38 |
| 江苏省 | 2.40 | 5.32 | 5.80 |
| 浙江省 | 1.85 | 1.40 | 2.79 |
| 安徽省 | 1.83 | 3.42 | 3.13 |
| 福建省 | 2.25 | 1.90 | 2.05 |
| 江西省 | 2.56 | 2.38 | 2.22 |
| 山东省 | 5.16 | 4.19 | 5.31 |
| 河南省 | 5.21 | 4.97 | 5.21 |
| 湖北省 | 1.92 | 2.93 | 2.52 |
| 湖南省 | 2.88 | 3.53 | 2.75 |
| 广东省 | 2.25 | 2.47 | 2.53 |
| 广西壮族自治区 | 1.29 | 2.10 | 1.64 |
| 海南省 | 1.34 | 1.57 | 1.92 |
| 重庆市 | 1.94 | 3.68 | 2.34 |
| 四川省 | 1.79 | 1.90 | 1.39 |
| 贵州省 | 1.79 | 1.71 | 1.73 |
| 云南省 | 0.58 | 0.97 | 0.94 |
| 西藏自治区 | 0.07 | 0.02 | 0.06 |
| 陕西省 | 1.75 | 1.18 | 1.43 |
| 甘肃省 | 0.62 | 0.46 | 0.53 |
| 青海省 | 0.10 | 0.05 | 0.08 |
| 宁夏回族自治区 | 0.54 | 0.38 | 0.64 |
| 新疆维吾尔自治区 | 0.10 | 0.12 | 0.10 |
| [1] |
杨少垒,刘涛,陈娟. 西部地区农村医疗卫生服务效率测度及动态分析[J]. 农村经济,2020(11):129-135.
|
| [2] |
周建再,代宝珍. 我国农村医疗卫生资源效率——基于省际面板数据的研究[J]. 华东经济管理,2014,28(9):54-58. DOI:10.3969/j.issn.1007-5097.2014.09.011.
|
| [3] | |
| [4] |
裴璇,俞佳立,钱芝网,等. 中国农村医疗卫生服务效率的区域差异研究[J]. 统计与决策,2022,38(22):40-45. DOI:10.13546/j.cnki.tjyjc.2022.22.008.
|
| [5] |
唐立健,王长青,钱东福. 江苏省农村医疗卫生资源配置现状及效率分析[J]. 中国卫生事业管理,2021,38(8):610-614.
|
| [6] |
林谋贵,兰韦娟,倪杰文,等. 我国农村村级卫生资源配置公平与效率分析[J]. 中国卫生经济,2023,42(2):53-57.
|
| [7] |
王慧慧,魏万宏,张传排,等. 河南省农村医疗卫生资源现状研究[J]. 中国卫生事业管理,2011,28(1):40-42. DOI:10.3969/j.issn.1004-4663.2011.01.015.
|
| [8] |
马斌,庞婷,郝桂芳. 山西省农村医疗卫生资源配置问题研究[J]. 系统科学学报,2013,21(2):75-77.
|
| [9] |
|
| [10] |
赵康普,马爽. 基于DEA的全国各地区基层卫生资源配置效率分析[J]. 中国医院,2021,25(12):27-30.
|
| [11] |
邓晓欣,姚中进. 我国三大重大战略区域的卫生资源配置效率分析[J]. 现代预防医学,2022,49(9):1631-1635.
|
| [12] |
陈琳,田晋莹,廖竞浩,等. 广东省21个城市卫生资源配置效率研究[J]. 中国卫生资源,2019,22(3):219-224.
|
| [13] |
袁素维,危凤卿,刘雯薇,等. 利用集聚度评价卫生资源配置公平性的方法学探讨[J]. 中国医院管理,2015,35(2):3-5.
|
| [14] |
范海龙,王碧艳. 基于集聚度和集中指数的广西区域卫生资源配置公平性分析[J]. 中国卫生资源,2022,25(6):829-834,841. DOI:10.13688/j.cnki.chr.2022.220349.
|
| [15] |
|
| [16] |
|
| [17] |
杨洁,庞震苗,徐庆锋,等. 基于集聚度和地理信息系统研究广东省中医药卫生资源公平性[J]. 实用医学杂志,2022,38(2):222-227. DOI:10.3969/j.issn.1006-5725.2022.02.018.
|
| [18] |
卢小兰,张可心. 武汉市卫生资源配置公平性与效率的时空特征研究[J]. 医学与社会,2021,34(9):16-21.
|
| [19] |
高凯丽,王紫红,高山. 基于DEA模型的我国中医医院运营效率的综合评价[J]. 现代预防医学,2022,49(4):690-694,705.
|
| [20] |
王锐,那丽,马月丹,等. 卫生健康高质量发展的内涵与路径选择[J]. 卫生经济研究,2022,39(7):1-4. DOI:10.14055/j.cnki.33-1056/f.2022.07.018.
|
| [21] |
张成,倪洁,巫抑扬,等. 基于DEA和Malmquist的四川省医疗服务产出效率研究[J]. 中国卫生统计,2022,39(2):263-266. DOI:10.3969/j.issn.1002-3674.2022.02.025.
|
| [22] |
甘明玉,张翔. 基于DEA和SFA方法的我国中医类医疗机构卫生资源配置效率评价研究[J]. 中国卫生事业管理,2021,38(9):676-679,712.
|
| [23] |
孙统达,李辉,王幸波,等. 共同富裕视域下卫生健康发展评价体系构建及实证研究[J]. 卫生经济研究,2022,39(9):5-9. DOI:10.14055/j.cnki.33-1056/f.2022.09.006.
|
| [24] |
王高玲,刘军军,严蓓蕾,等. 基于集聚度和GIS技术的江苏省医疗卫生资源公平性分析[J]. 中国卫生统计,2020,37(6):888-891. DOI:10.3969/j.issn.1002-3674.2020.06.022.
|
| [25] | |
| [26] |
赵雪雁,王晓琪,刘江华,等. 基于不同尺度的中国优质医疗资源区域差异研究[J]. 经济地理,2020,40(7):22-31. DOI:10.15957/j.cnki.jjdl.2020.07.003.
|
| [27] | |
| [28] |
廖成中,毛磊,翟坤周. 共同富裕导向下东西部协作赋能乡村振兴:机理、模式与策略[J]. 改革,2022(10):91-105.
|
| [29] |
艾晓倩,乔学斌,徐爱军. 基于DEA的全国中医类医疗机构卫生资源配置效率评价[J]. 中国农村卫生事业管理,2022,42(1):27-32,36. DOI:10.19955/j.cnki.1005-5916.2022.01.005.
|
| [1] | 张冰清, 王忠凯, 吴长勇, 孙煌, 李锐洁, 刘文洁, 骆怡哗, 郑丽慧, 彭云珠. 1990—2021年全球先天性心脏缺陷疾病负担变化及未来趋势预测研究[J]. 中国全科医学, 2025, 28(18): 2253-2261. |
| [2] | 史穆然, 武宁, 宋丽娟. 我国中医全科医生队伍发展现状及统计优化建议[J]. 中国全科医学, 2025, 28(13): 1560-1566. |
| [3] | 王金震, 李俊, 陆冬春, 李家顺, 江雁, 聂莲莲, 杨旦红. 基于地理信息系统的家庭医生签约服务平台开发与可用性评价[J]. 中国全科医学, 2025, 28(10): 1236-1242. |
| [4] | 杨旦红, 李俊, 李锋, 李俊磊, 何芳, 鲁叶花, 王金震, 江雁. 基于地理信息系统的家庭医生信息服务平台应用[J]. 中国全科医学, 2025, 28(10): 1243-1248. |
| [5] | 刘海燕, 宁艳花, 孔维娟, 郭亚红, 史晶, 柳玲娜, 吕兄兄, 李美曼. 我国农村家庭医生签约服务老年人健康管理实践影响因素:一项范围综述[J]. 中国全科医学, 2025, 28(04): 482-490. |
| [6] | 谢坤, 王萱萱, 李思清, 高淑红, 陈家应, 张朝阳. 我国农村医生社区健康管理能力调查研究[J]. 中国全科医学, 2024, 27(34): 4308-4314. |
| [7] | 邱林萍, 宋国强, 刘梦, 姜城蕾, 孙先红. 我国省间基层医疗卫生机构医护资源分布特征研究[J]. 中国全科医学, 2024, 27(31): 3911-3918. |
| [8] | 李筱纯, 郝模, 李程跃, 蒲川. 重庆市慢性病防控资源配置适宜程度研究[J]. 中国全科医学, 2024, 27(25): 3178-3183. |
| [9] | 李丽清, 刘文慧, 杨苏乐, 林慧英. 基层医疗资源配置与经济高质量发展的耦合协调及其预测分析[J]. 中国全科医学, 2024, 27(25): 3164-3170. |
| [10] | 张兰, 张瑞华, 吴雪莲, 杨燕, 段桂敏, 赵大仁. 中国西部地区全科医生资源配置公平性分析及需求预测研究[J]. 中国全科医学, 2024, 27(25): 3171-3177. |
| [11] | 刘影, 姜俊丞, 景汇泉. 我国中老年人群慢性病患病率及患病种类区域差异与医疗卫生资源的相关性研究[J]. 中国全科医学, 2024, 27(12): 1452-1459. |
| [12] | 李娅玲, 顾燕峰, 郑艳玲, 蔡学民, 王伟, 余海燕, 杜兆辉. 城市社区卫生服务中心发展情况调查研究[J]. 中国全科医学, 2024, 27(10): 1166-1172. |
| [13] | 刘影, 姜俊丞, 景汇泉. 我国东、中、西部地区中老年人失能及其影响因素的区域差异研究[J]. 中国全科医学, 2024, 27(07): 877-885. |
| [14] | 李丽清, 杨苏乐, 万里晗, 卢祖洵. 基于fsQCA组态视角的我国医疗资源配置效率提升路径分析[J]. 中国全科医学, 2024, 27(04): 413-419. |
| [15] | 张峥岩, 王振中, 张伋, 宫恩莹, 邵瑞太. 医疗保健生态学模型在卫生服务研究中的应用现状及启示:一项概况性评价[J]. 中国全科医学, 2024, 27(04): 391-399. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||










