中国全科医学 ›› 2024, Vol. 27 ›› Issue (20): 2505-2511.DOI: 10.12114/j.issn.1007-9572.2023.0614
王萧冉, 关新月, 张丹*( )
)
WANG Xiaoran, GUAN Xinyue, ZHANG Dan*()
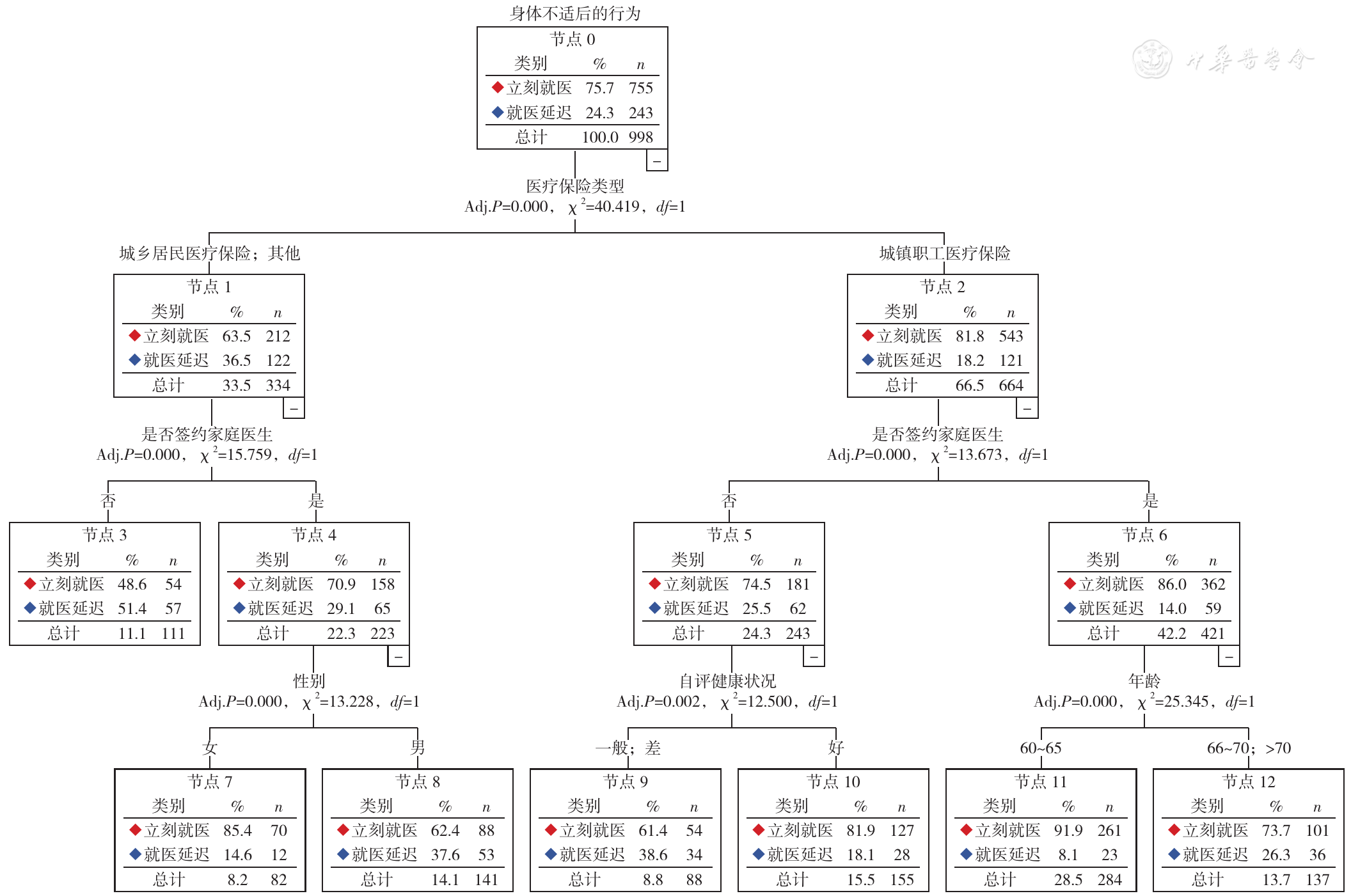
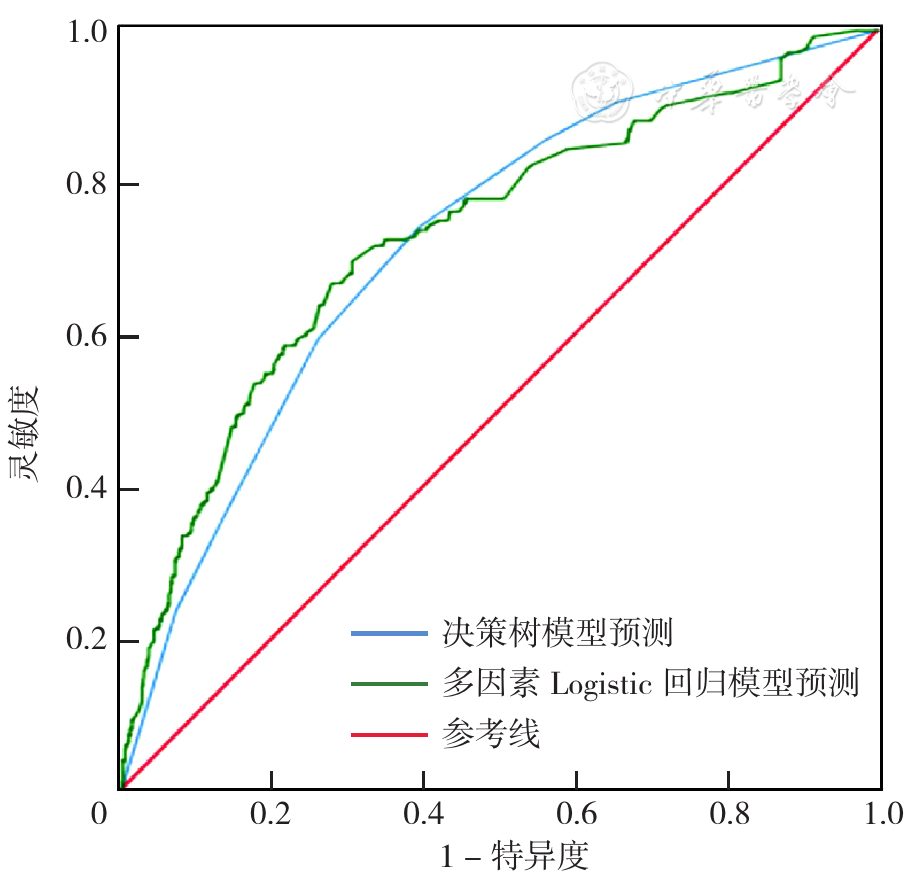
摘要: 背景 随着我国人口老龄化的加剧,居民疾病谱发生变化,多种慢性病共存成为我国老年群体健康状况的常态。就医延迟是指个体在身体不适后由于各种主观或客观原因未能及时就医的行为,导致治疗效果下降、患者生存质量降低。目前,国内针对老年慢性病共病患者就医延迟行为及其影响因素的研究较少。目的 探讨老年慢性病共病患者就医延迟行为及其影响因素,为进一步改善老年共病患者就医延迟行为提供参考。方法 采用多阶段分层整群随机抽样法,选取2022年9—12月于广东省27个社区卫生服务中心就诊的符合条件的老年共病患者作为研究对象。采用自行设计的调查问卷收集患者的一般资料、疾病相关资料和就医延迟情况。采用多因素Logistic回归分析和基于CHAID算法的决策树模型分析老年共病患者就医延迟行为的影响因素。结果 共纳入研究对象998例,其中出现就医延迟行为243例(24.35%)。多因素Logistic回归分析结果显示,性别(女性:OR=0.701,95%CI=0.504~0.977,P=0.036)、户籍类型(农村:OR=0.590,95%CI=0.358~0.973,P=0.039)、医疗保险类型(城乡居民医疗保险:OR=2.660,95%CI=1.764~4.010,P<0.001)、疾病相关自我效能(低:OR=4.378,95%CI=2.079~9.217,P<0.001)、是否签约家庭医生(否:OR=2.277,95%CI=1.618~3.206,P<0.001)、自评健康状况(一般:OR=1.554,95%CI=1.073~2.250,P=0.020)是老年共病患者就医延迟行为的影响因素。决策树模型共3层,13个节点,共筛选出医疗保险类型、是否签约家庭医生、性别、自评健康状况、年龄5个影响因素。两种模型预测老年共病患者就医延迟行为的结果显示,多因素Logistic回归模型的受试者工作特征曲线下面积(AUC)为0.729,决策树模型的AUC为0.721。两种模型对老年共病患者就医延迟行为的预测效果的AUC比较,差异无统计学意义(Z=0.539,P=0.590)。结论 广东省老年共病患者就医延迟行为发生率为24.35%,医疗保险类型、家庭医生签约率、性别与疾病自评健康状况是老年共患者发生就医延迟行为的主要影响因素。应进一步完善医疗保障制度,提高家庭医生签约率与利用率,进而降低就医延迟行为发生率。