中国全科医学 ›› 2024, Vol. 27 ›› Issue (03): 315-321.DOI: 10.12114/j.issn.1007-9572.2023.0395
所属专题: 阿尔茨海默病最新文章合辑; 老年人群健康最新文章合辑; 老年问题最新文章合辑; 脑健康最新研究合辑
王英1,2,3, 董之晓4, 杨克虎2,*( )
)
WANG Ying1,2,3, DONG Zhixiao4, YANG Kehu2,*()
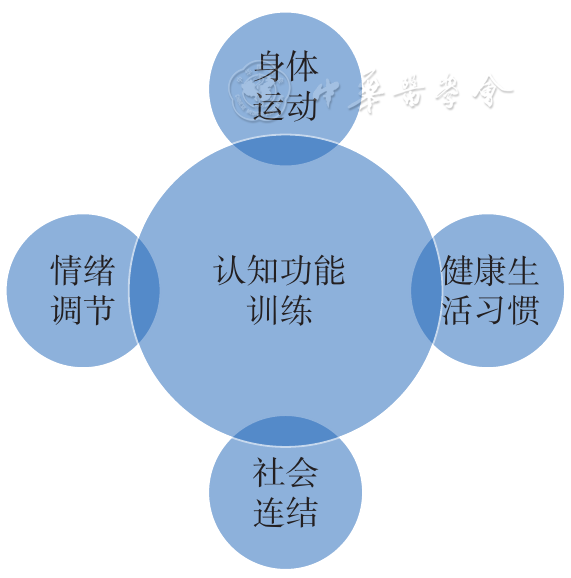
摘要: 背景 认知障碍可导致老年人认知功能下降、抑郁、孤独感,以及自我效能感和生活质量的下降。 目的 探讨非药物整合式干预对轻度老年认知障碍患者认知功能、抑郁、孤独感、自我效能感和生活质量的干预效果。 方法 基于认知障碍的风险因素研发了认知功能训练、身体运动、情绪管理、社会连结、健康生活习惯5个维度的非药物整合式干预方案,采用A-B-A单个案受试者设计,于2021年6—12月展开对3名确诊为轻度认知障碍的老年人进行为期3个月,1次/周,60 min/次的干预。于基线、干预3个月后、干预结束后3个月时采用蒙特利尔认知评估量表(MoCA)、自我效能感量表(GSES)、简版生活质量量表(SF-12)、简版老年抑郁量表(GDS-15)、中文版孤独量表(DJGLS)从认知功能、自我效能感、生活质量、抑郁情绪、孤独感5个维度评估3名老年人各量表得分并分析其变化。并在干预结束后3个月进行半结构式访谈,从认知功能、生活质量、抑郁情绪、自我效能感和孤独感维度评估干预效果。 结果 纳入研究的3名老年人年龄为74、70、73岁,均已婚、与配偶和孙辈共同居住。3名老年人的MoCA基线得分为21、22、24分,干预3个月后为28、26、27分,干预结束后3个月为25、19、23分;GSES基线得分为25、30、27分,干预3个月后为29、29、30分,干预结束后3个月为28、31、28分。SF-12基线时得分为69、32、51分,干预3个月后为81、81、83分,干预结束后3个月为78、38、59分。GDS-15基线得分为4、8、2分,干预3个月后为2、6、1分,干预结束后3个月为1、8、4分。DJGLS基线得分为8、7、8分,干预3个月后为5、5、4分,干预结束后3个月为5、5、7分。半结构访谈资料表明,受试者在认知功能、生活质量、抑郁情绪、孤独感、自我效能感5个维度均有改善。 结论 对于患有轻度老年认知障碍的受试老年人而言,从认知功能训练、身体运动、情绪调节、社会连结、健康生活习惯5个维度开展非药物整合式的干预是有意义的,轻度老年认知障碍老年人的MoCA、SF-12、GDS-15、DJGLS得分在干预3个月后均有改善,GSES得分在干预后效果不理想,所有维度得分在干预结束后3个月呈递减趋势。