
中国全科医学 ›› 2024, Vol. 27 ›› Issue (01): 15-26.DOI: 10.12114/j.issn.1007-9572.2022.0852
所属专题: 指南/共识最新文章合辑; 心理健康最新文章合辑
Searle Kendall1,*( ), Blashki Grant2, Kakuma Ritsuko3, 杨辉4, 吕淑荣2, 李宝琪5, 肖莹莹5, Minas Harry1
), Blashki Grant2, Kakuma Ritsuko3, 杨辉4, 吕淑荣2, 李宝琪5, 肖莹莹5, Minas Harry1
收稿日期:2023-04-26
修回日期:2023-07-25
出版日期:2024-01-05
发布日期:2023-10-23
通讯作者:
Searle Kendall
Searle Kendall1,*(), Blashki Grant2, Kakuma Ritsuko3, YANG Hui4, LYU Shurong2, LI Baoqi5, XIAO Yingying5, Minas Harry1
Received:2023-04-26
Revised:2023-07-25
Published:2024-01-05
Online:2023-10-23
Contact:
Searle Kendall
摘要: 背景 中国全科医生越来越期望能够识别和预防抑郁障碍,但其接受的心理健康培训有限,社区卫生服务中心(CHCs)也缺乏针对抑郁障碍的诊断和服务规范。WHO《心理健康差距干预指南》第2版(mhGAP-IG.v2)是为非心理健康专业人员提供的决策支持工具,可用于评估、管理、随访精神障碍、神经疾病及物质使用障碍患者。鉴于mhGAP-IG.v2的通用性,其在中国的应用应根据抑郁障碍在不同文化下的差异性和中国心理健康系统特点进行调整。 方法 开展两轮基于网络的德尔菲(Delphi)调查。邀请来自深圳市的全科医生小组对mhGAP-IG.v2中涉及抑郁障碍的199条表述进行五分制的赞同程度打分,即"如要把该表述用在深圳市,是否赞同调整其内容和结构"。如果>80%的全科医生"有些/肯定赞同"调整某表述,则视为全科医生对调整该表述达成共识;如果>80%的全科医生"有些/肯定不赞同"调整某表述,则视为全科医生对不调整该表述达成共识。 结果 全科医生对79%的表述达成了需要调整的共识,平均得分为4.26分,即全科医生"有些赞同"对mhGAP-IG.v2中涉及抑郁障碍的相关表述进行调整。具体调整建议包括:抑郁评估方法应考虑更广泛的抑郁症状,并考虑病情的发展阶段;增加抑郁筛查工具的使用指南;明确全科医生的作用,以及家庭参与和跨部门服务的转诊途径;药物治疗建议应与中国用药规范保持一致;指南所有章节要强调预防自杀;情境化健康教育;强调"以人为本"的服务方法。全科医生认为,应维持mhGAP-IG.v2中对经历抑郁发作的双相障碍患者的诊断和治疗建议。 结论 对mhGAP-IG.v2抑郁部分的调整研究反映出对指南的评估应考虑文化和国情背景,包括中国特色的初级卫生保健系统、健康优先领域、治疗可得性,以及多样化的社会心理教育需要。调整后的mhGAP-IG.v2可以给中国全科医学教育和全科医疗服务提供参考,也可以为其他国家的非精神病学专业人员开展心理健康服务提供有益借鉴。
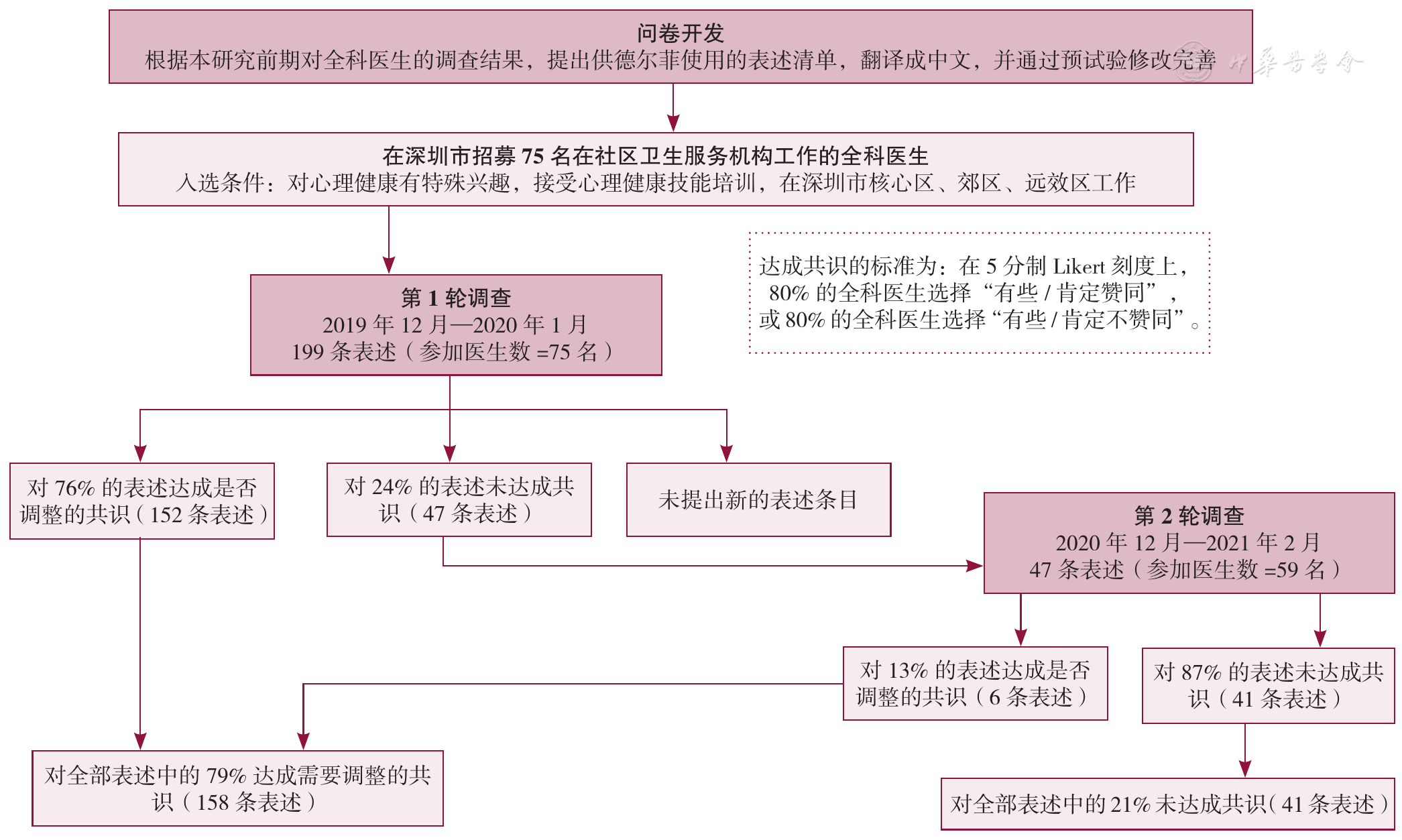
图1 从问卷开发到达成是否需要调整共识的德尔菲过程
Figure 1 Delphi process from questionnaire development to statement consensus
| mhGAP-IG.v2中涉及抑郁的主题 | 第1轮(n=75) | 第2轮(n=59) | 总体共识 | |||||
|---|---|---|---|---|---|---|---|---|
| 表述条目数(条) | 达成调整共识的条目(%) | 平均分(分) | 表述条目数(条) | 达成调整共识的条目(%) | 平均分(分) | 达成调整共识的条目(%) | 平均分(分) | |
| "以人为本"的指南 | 18 | 100 | 4.65 | 0 | 0 | 0 | 100 | 4.65 |
| 抑郁障碍的表现特征 | 28 | 64 | 4.07 | 10 | 0 | 3.50 | 64 | 4.06 |
| 筛查工具的获得和使用 | 11 | 64 | 4.13 | 4 | 25 | 3.80 | 73 | 4.24 |
| 医疗服务及社区系统的内部关系 | 28 | 79 | 4.23 | 6 | 17 | 3.75 | 82 | 4.26 |
| 药物治疗选择 | 18 | 78 | 4.20 | 4 | 0 | 3.51 | 78 | 4.19 |
| 双相障碍中的躁狂和抑郁发作 | 4 | 100 | 4.59 | 0 | 0 | 0 | 100 | 4.59 |
| 与患者和社区针对抑郁进行沟通 | 29 | 90 | 4.36 | 3 | 0 | 3.77 | 90 | 4.36 |
| 随访 | 33 | 61 | 4.03 | 13 | 31 | 3.64 | 73 | 4.05 |
| 管理患者信息 | 11 | 82 | 4.20 | 2 | 0 | 3.73 | 82 | 4.20 |
| 指南的整体结构 | 19 | 74 | 4.06 | 5 | 0 | 3.61 | 74 | 4.06 |
| 总体共识 | 199 | 76 | 4.25 | 47 | 13 | 3.66 | 79 | 4.26 |
表1 按主题划分的第1轮和第2轮德尔菲调查获得的共识
Table 1 Wave 1 & 2 Delphi survey consensus by thematic domains
| mhGAP-IG.v2中涉及抑郁的主题 | 第1轮(n=75) | 第2轮(n=59) | 总体共识 | |||||
|---|---|---|---|---|---|---|---|---|
| 表述条目数(条) | 达成调整共识的条目(%) | 平均分(分) | 表述条目数(条) | 达成调整共识的条目(%) | 平均分(分) | 达成调整共识的条目(%) | 平均分(分) | |
| "以人为本"的指南 | 18 | 100 | 4.65 | 0 | 0 | 0 | 100 | 4.65 |
| 抑郁障碍的表现特征 | 28 | 64 | 4.07 | 10 | 0 | 3.50 | 64 | 4.06 |
| 筛查工具的获得和使用 | 11 | 64 | 4.13 | 4 | 25 | 3.80 | 73 | 4.24 |
| 医疗服务及社区系统的内部关系 | 28 | 79 | 4.23 | 6 | 17 | 3.75 | 82 | 4.26 |
| 药物治疗选择 | 18 | 78 | 4.20 | 4 | 0 | 3.51 | 78 | 4.19 |
| 双相障碍中的躁狂和抑郁发作 | 4 | 100 | 4.59 | 0 | 0 | 0 | 100 | 4.59 |
| 与患者和社区针对抑郁进行沟通 | 29 | 90 | 4.36 | 3 | 0 | 3.77 | 90 | 4.36 |
| 随访 | 33 | 61 | 4.03 | 13 | 31 | 3.64 | 73 | 4.05 |
| 管理患者信息 | 11 | 82 | 4.20 | 2 | 0 | 3.73 | 82 | 4.20 |
| 指南的整体结构 | 19 | 74 | 4.06 | 5 | 0 | 3.61 | 74 | 4.06 |
| 总体共识 | 199 | 76 | 4.25 | 47 | 13 | 3.66 | 79 | 4.26 |
| 主题 | mhGAP-IG.v2的调整建议 |
|---|---|
| 1."以人为本"的指南 | 1.1不仅是"以患者为中心",而且要强调"以人为本" |
| -确切保护患者隐私 | |
| -对患者的生活事件(如悲伤)保持敏感 | |
| -适应患者的多样性 | |
| 1.2提供个体化的患者管理计划(PMP) | |
| -与患者建立伙伴关系 | |
| -保持随时间发展的灵活性,以满足患者需要 | |
| -列出可以激发出积极的行为改变的几种策略 | |
| 1.3使PMP与医生、患者、业务管理相匹配 | |
| -医生评估治疗进展(如评估药物副作用,改变治疗方法) | |
| -患者对治疗的评价(如对治疗的体验、对治疗的参与) | |
| -业务跟踪(如预约就诊、可能的转诊选项) | |
| 1.4由有心理健康服务证书的全科医生制定PMP框架 | |
| 1.5解决背景不同的问题 | |
| -优先考虑自杀风险 | |
| -在每个服务阶段强调家庭参与 | |
| -提供深圳市患者治疗成功的案例 | |
| 2.双相障碍中的躁狂和抑郁发作 | 2.1区分非复杂抑郁与双相障碍(抑郁发作)在治疗方法上的不同 |
| -把心境稳定剂作为抗抑郁药的辅助用药 | |
| 2.2与患者或家属一起,核查躁狂的症状 | |
| 3.与患者和社区针对抑郁进行沟通 | 3.1医生发挥提高社区意识和健康素养的作用 |
| 3.2更强调家庭在患者支持上的作用 | |
| 3.3将监督有自杀风险患者纳入社区卫生服务中心工作范畴 | |
| 3.4充实患者心理教育的内容 | |
| -纳入培养患者信任的策略(如赋予同理心的倾听) | |
| -纠正任何对疾病的误解 | |
| -提供治疗成功的案例故事 | |
| -让患者准备好应对社区的抑郁污名化 | |
| -讨论治疗依从性的重要性 | |
| -提供参与治疗活动的建议 | |
| -鼓励参加社区卫生服务中心随访和专家随诊 | |
| -与患者达成管理/医疗服务计划的共识 | |
| -提供自我管理的建议 | |
| 3.5考虑实施预约系统 | |
| 4.医疗服务及社区系统的内部关系 | 4.1强调社区参与对自杀风险患者的监督 |
| 4.2明确转诊路径,以及各种职业之间的责任分工 | |
| 4.3强调医学和非医学跨领域服务的机会 | |
| 4.4把家庭参与作为跨领域服务的一部分 | |
| 4.5加上提醒,把患者置于所有讨论的核心 | |
| 5.筛查工具的获得和使用 | 5.1推荐在管理和/或随诊时使用的问卷 |
| 5.2在私密诊室使用问卷 | |
| 5.3医生和护士都能使用问卷(假设提供过培训) | |
| 5.4明确工具范围(多次使用?非临床场所使用?) | |
| 6.管理患者信息 | 6.1看诊前回顾病史,并更新病史记录 |
| 6.2如果需要,补充患者管理系统的信息 | |
| 6.3通过专家、其他治疗医生、家庭成员反馈及评估用药反应等,证实治疗效果 | |
| 6.4定期召开诊所内会议,与其他医生讨论疑难病例 | |
| 7.药物治疗选择 | 7.1在监督和更改药物剂量时,说明医生的任务 |
| 7.2加上每种药物的用药指征和副反应 | |
| 7.3加上每种药物的可得性和医保报销情况 | |
| 7.4加上每种药物的依从建议 | |
| 7.5提供最新药物的详细信息 | |
| 7.6提供药物的商品名举例 | |
| 7.7增加苯二氮 | |
| 8.抑郁障碍的表现特征 | 8.1指南应"反映真实的看诊情况" |
| -考虑患者是否以往有过抑郁发作 | |
| -明确关系问题的细节(包括悲伤) | |
| -在看诊的早期评估患者的自杀风险 | |
| -首先考虑躯体症状 | |
| 8.2包括抑郁的触发因素和风险因素 | |
| 8.3根据"一系列症状,而非核心症状"做出诊断 | |
| -在症状清单中同时列出核心症状和其他症状 | |
| -在症状清单中纳入性欲减退 | |
| -按照是否能更好地预测抑郁/常见症状,列出症状 | |
| -提供随时间变化的症状的额外详细信息 | |
| 8.4在结构上澄清躯体症状和心理症状之间的不同 | |
| 8.5儿童患者需要的额外症状信息 | |
| 8.6谨慎地量化/翻译如下表述 | |
| -"睡眠过多" | |
| -"比平常讲话和活动缓慢" | |
| 9.指南的整体结构 | 9.1为更好地反映应用的背景条件,需要随结构进行某些或较大的重组 |
| 9.2强调跨领域参与,包括家庭/社区网络 | |
| 9.3强调一般抑郁与双相障碍(抑郁发作)之间的不同 | |
| 9.4将随诊和管理整合进一个连续的部分 | |
| 9.5在开始评估时,考虑到高自杀风险患者 | |
| 9.6将患者作为指南的核心 | |
| 10.随访 | 10.1确定随诊,并解释为什么随诊是必要的 |
| -确定患者的治疗状态 | |
| -确定患者以往接受的治疗 | |
| -监测当前治疗的副反应,并评估改善情况 | |
| 10.2解释怎样评估进展,即逐项列出改善的征象 | |
| 10.3强调社区卫生服务中心在随诊中要达到的主要结果 | |
| -在社区卫生服务中心层面,基本心理治疗的选项 | |
| -心理干预/药物治疗的转诊选项 | |
| 10.4逐项列出随诊的联系方式(面对面、电话、电子化) | |
| 10.5推荐首选看诊方式 | |
| -理想的,对所有患者进行面对面随诊 | |
| -至少,对病情严重患者进行面对面随诊 | |
| -患者对非紧急情况的看诊偏好 | |
| 10.6根据抑郁的严重程度、自残风险、治疗依从程度,确定随诊的频率和持续时间 |
表2 全科医生对mhGAP-IG.v2条目的调整建议
Table 2 Primary care recommendations for an adapted mhGAP-IG.v2
| 主题 | mhGAP-IG.v2的调整建议 |
|---|---|
| 1."以人为本"的指南 | 1.1不仅是"以患者为中心",而且要强调"以人为本" |
| -确切保护患者隐私 | |
| -对患者的生活事件(如悲伤)保持敏感 | |
| -适应患者的多样性 | |
| 1.2提供个体化的患者管理计划(PMP) | |
| -与患者建立伙伴关系 | |
| -保持随时间发展的灵活性,以满足患者需要 | |
| -列出可以激发出积极的行为改变的几种策略 | |
| 1.3使PMP与医生、患者、业务管理相匹配 | |
| -医生评估治疗进展(如评估药物副作用,改变治疗方法) | |
| -患者对治疗的评价(如对治疗的体验、对治疗的参与) | |
| -业务跟踪(如预约就诊、可能的转诊选项) | |
| 1.4由有心理健康服务证书的全科医生制定PMP框架 | |
| 1.5解决背景不同的问题 | |
| -优先考虑自杀风险 | |
| -在每个服务阶段强调家庭参与 | |
| -提供深圳市患者治疗成功的案例 | |
| 2.双相障碍中的躁狂和抑郁发作 | 2.1区分非复杂抑郁与双相障碍(抑郁发作)在治疗方法上的不同 |
| -把心境稳定剂作为抗抑郁药的辅助用药 | |
| 2.2与患者或家属一起,核查躁狂的症状 | |
| 3.与患者和社区针对抑郁进行沟通 | 3.1医生发挥提高社区意识和健康素养的作用 |
| 3.2更强调家庭在患者支持上的作用 | |
| 3.3将监督有自杀风险患者纳入社区卫生服务中心工作范畴 | |
| 3.4充实患者心理教育的内容 | |
| -纳入培养患者信任的策略(如赋予同理心的倾听) | |
| -纠正任何对疾病的误解 | |
| -提供治疗成功的案例故事 | |
| -让患者准备好应对社区的抑郁污名化 | |
| -讨论治疗依从性的重要性 | |
| -提供参与治疗活动的建议 | |
| -鼓励参加社区卫生服务中心随访和专家随诊 | |
| -与患者达成管理/医疗服务计划的共识 | |
| -提供自我管理的建议 | |
| 3.5考虑实施预约系统 | |
| 4.医疗服务及社区系统的内部关系 | 4.1强调社区参与对自杀风险患者的监督 |
| 4.2明确转诊路径,以及各种职业之间的责任分工 | |
| 4.3强调医学和非医学跨领域服务的机会 | |
| 4.4把家庭参与作为跨领域服务的一部分 | |
| 4.5加上提醒,把患者置于所有讨论的核心 | |
| 5.筛查工具的获得和使用 | 5.1推荐在管理和/或随诊时使用的问卷 |
| 5.2在私密诊室使用问卷 | |
| 5.3医生和护士都能使用问卷(假设提供过培训) | |
| 5.4明确工具范围(多次使用?非临床场所使用?) | |
| 6.管理患者信息 | 6.1看诊前回顾病史,并更新病史记录 |
| 6.2如果需要,补充患者管理系统的信息 | |
| 6.3通过专家、其他治疗医生、家庭成员反馈及评估用药反应等,证实治疗效果 | |
| 6.4定期召开诊所内会议,与其他医生讨论疑难病例 | |
| 7.药物治疗选择 | 7.1在监督和更改药物剂量时,说明医生的任务 |
| 7.2加上每种药物的用药指征和副反应 | |
| 7.3加上每种药物的可得性和医保报销情况 | |
| 7.4加上每种药物的依从建议 | |
| 7.5提供最新药物的详细信息 | |
| 7.6提供药物的商品名举例 | |
| 7.7增加苯二氮 | |
| 8.抑郁障碍的表现特征 | 8.1指南应"反映真实的看诊情况" |
| -考虑患者是否以往有过抑郁发作 | |
| -明确关系问题的细节(包括悲伤) | |
| -在看诊的早期评估患者的自杀风险 | |
| -首先考虑躯体症状 | |
| 8.2包括抑郁的触发因素和风险因素 | |
| 8.3根据"一系列症状,而非核心症状"做出诊断 | |
| -在症状清单中同时列出核心症状和其他症状 | |
| -在症状清单中纳入性欲减退 | |
| -按照是否能更好地预测抑郁/常见症状,列出症状 | |
| -提供随时间变化的症状的额外详细信息 | |
| 8.4在结构上澄清躯体症状和心理症状之间的不同 | |
| 8.5儿童患者需要的额外症状信息 | |
| 8.6谨慎地量化/翻译如下表述 | |
| -"睡眠过多" | |
| -"比平常讲话和活动缓慢" | |
| 9.指南的整体结构 | 9.1为更好地反映应用的背景条件,需要随结构进行某些或较大的重组 |
| 9.2强调跨领域参与,包括家庭/社区网络 | |
| 9.3强调一般抑郁与双相障碍(抑郁发作)之间的不同 | |
| 9.4将随诊和管理整合进一个连续的部分 | |
| 9.5在开始评估时,考虑到高自杀风险患者 | |
| 9.6将患者作为指南的核心 | |
| 10.随访 | 10.1确定随诊,并解释为什么随诊是必要的 |
| -确定患者的治疗状态 | |
| -确定患者以往接受的治疗 | |
| -监测当前治疗的副反应,并评估改善情况 | |
| 10.2解释怎样评估进展,即逐项列出改善的征象 | |
| 10.3强调社区卫生服务中心在随诊中要达到的主要结果 | |
| -在社区卫生服务中心层面,基本心理治疗的选项 | |
| -心理干预/药物治疗的转诊选项 | |
| 10.4逐项列出随诊的联系方式(面对面、电话、电子化) | |
| 10.5推荐首选看诊方式 | |
| -理想的,对所有患者进行面对面随诊 | |
| -至少,对病情严重患者进行面对面随诊 | |
| -患者对非紧急情况的看诊偏好 | |
| 10.6根据抑郁的严重程度、自残风险、治疗依从程度,确定随诊的频率和持续时间 |
| [1] |
深圳市统计局,深圳市第七次全国人口普查领导小组办公室. 深圳市第七次全国人口普查公报[A/OL]. (2021-05-17)[2022-01-05].
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
中共中央,国务院. "健康中国2030"规划纲要[A/OL]. (2016-10-25)[2022-01-05].
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
WHO. mhGAP intervention guide for mental,neurological and substance use disorders in non-specialized health settings:mental health gap action programme(mhGAP)[M]. Geneva:World Health Organization,2010.
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
WHO. mhGAP intervention guide for mental,neurological and substance use disorder in non-specialised health settings[M]. 2nd ed. Geneva:World Health Organization,2016.
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [42] |
|
| [43] |
|
| [44] |
|
| [45] |
|
| [46] |
|
| [47] |
|
| [48] |
|
| [49] |
|
| [50] |
|
| [51] |
|
| [52] |
|
| [53] |
|
| [54] |
|
| [55] |
|
| [56] |
|
| [57] |
|
| [58] |
|
| [59] |
|
| [60] |
|
| [61] |
|
| [62] |
|
| [63] |
|
| [64] |
|
| [65] |
|
| [66] |
|
| [67] |
|
| [68] |
|
| [69] |
World Health Organization. Framework on integrated,people-centred health services[R]. Geneva:World Health Organization,2016.
|
| [70] |
World Health Organization. Framework on integrated people-centred health services:an overview[EB/OL]. [2022-01-05].
|
| [71] |
|
| [72] |
|
| [73] |
|
| [74] |
|
| [75] |
|
| [76] |
|
| [77] |
|
| [78] |
|
| [79] |
|
| [80] |
|
| [1] | 尚忠华, 蒋芝月, 黄朝晖, 杨星, 刘海燕, 张丽. 1990—2021年中国宫颈癌疾病负担趋势分析及2022—2035年预测研究[J]. 中国全科医学, 2025, 28(26): 3314-3320. |
| [2] | 罗新宇, 刘瑾, 陈海龙. 1990—2021年中国和全球胰腺炎疾病负担趋势分析及2022—2031年预测研究[J]. 中国全科医学, 2025, 28(26): 3321-3327. |
| [3] | 褚艺婧, 严雨格, 顾杰, 席彪, 祝墡珠, 黄蛟灵. 中国基层医务人员留用意愿影响因素分析:基于城乡差异比较[J]. 中国全科医学, 2025, 28(25): 3161-3168. |
| [4] | 赵稳稳, 李诺雅, 张雅丽, 张金佳, 张敏, 刘华雷, 席彪, 王荣英. 临床住培基地(综合医院)全科医学师资质量评价指标体系构建研究[J]. 中国全科医学, 2025, 28(25): 3187-3192. |
| [5] | 胡婉琴, 余深艳, 曹学华, 向凤, 贾钰. 中国儿童性早熟影响因素的Meta分析[J]. 中国全科医学, 2025, 28(21): 2661-2671. |
| [6] | 郭艺, 韩烜烨, 刘昭君, 姜尧尧, 付洋, 石磊, 赵士宏. 基于E-Coach管理模式的儿童多重慢病医疗过渡干预模型构建研究[J]. 中国全科医学, 2025, 28(20): 2530-2537. |
| [7] | 朱立国. 夯实基层骨健康服务根基 助力推进健康中国计划[J]. 中国全科医学, 2025, 28(19): 2345-2345. |
| [8] | 魏戌, 尹煜辉, 王旭, 于若文, 章轶立, 孙凯, 王辉, 谢世明, 李琰, 秦晓宽, 尹逊路, 李玲慧, 朱立国. 基层医疗卫生机构骨健康服务能力评价指标体系研究[J]. 中国全科医学, 2025, 28(19): 2354-2362. |
| [9] | 陆唯怡, 张舒娴, 马冲, 石建伟. 基于德尔菲法的机构健康科普工作评价指标体系构建研究[J]. 中国全科医学, 2025, 28(18): 2307-2313. |
| [10] | 樊宇, 李蓉, 龚双英, 杨小娟, 李蕊. 中国产妇配偶产后抑郁发生率的Meta分析[J]. 中国全科医学, 2025, 28(17): 2179-2185. |
| [11] | 陈兴超, 高振华, 徐生刚, 邹永刚, 钱军, 魏建仝. 1990—2021年全球和中国及不同社会人口学指数地区骨关节炎疾病负担趋势分析[J]. 中国全科医学, 2025, 28(17): 2172-2178. |
| [12] | 令垚, 张文滨, 王仕鸿, 陈永泽, 董文娇, 邓星妤, 丁元林. 1990—2021年中国类风湿关节炎疾病负担变化趋势分析及预测研究[J]. 中国全科医学, 2025, 28(15): 1914-1922. |
| [13] | 陈沂, 白文佩, 李宏田, 王尧, 田宗梅, 顾蓓, 刘晓红, 杨慕坤. 绝经女性健康管理综合评估指标体系的构建研究[J]. 中国全科医学, 2025, 28(14): 1781-1787. |
| [14] | 孙清, 吴玉霄, 崔立敏. 中国2型糖尿病患者肌少-骨质疏松症患病率的Meta分析[J]. 中国全科医学, 2025, 28(12): 1520-1526. |
| [15] | 徐浩, 方达, 周卫红, 毕艳, 顾天伟. 中国内脏脂肪指数与脂肪肝发生风险的回顾性队列研究[J]. 中国全科医学, 2025, 28(11): 1336-1341. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||










