中国全科医学 ›› 2023, Vol. 26 ›› Issue (26): 3246-3251.DOI: 10.12114/j.issn.1007-9572.2023.0183
所属专题: 内分泌代谢性疾病最新文章合辑; 心力衰竭最新文章合辑; 心房颤动最新文章合辑
费思杰, 张强*( ), 刘方方, 白璐, 孙彩红, 信彩凤
), 刘方方, 白璐, 孙彩红, 信彩凤
FEI Sijie, ZHANG Qiang*(), LIU Fangfang, BAI Lu, SUN Caihong, XIN Caifeng
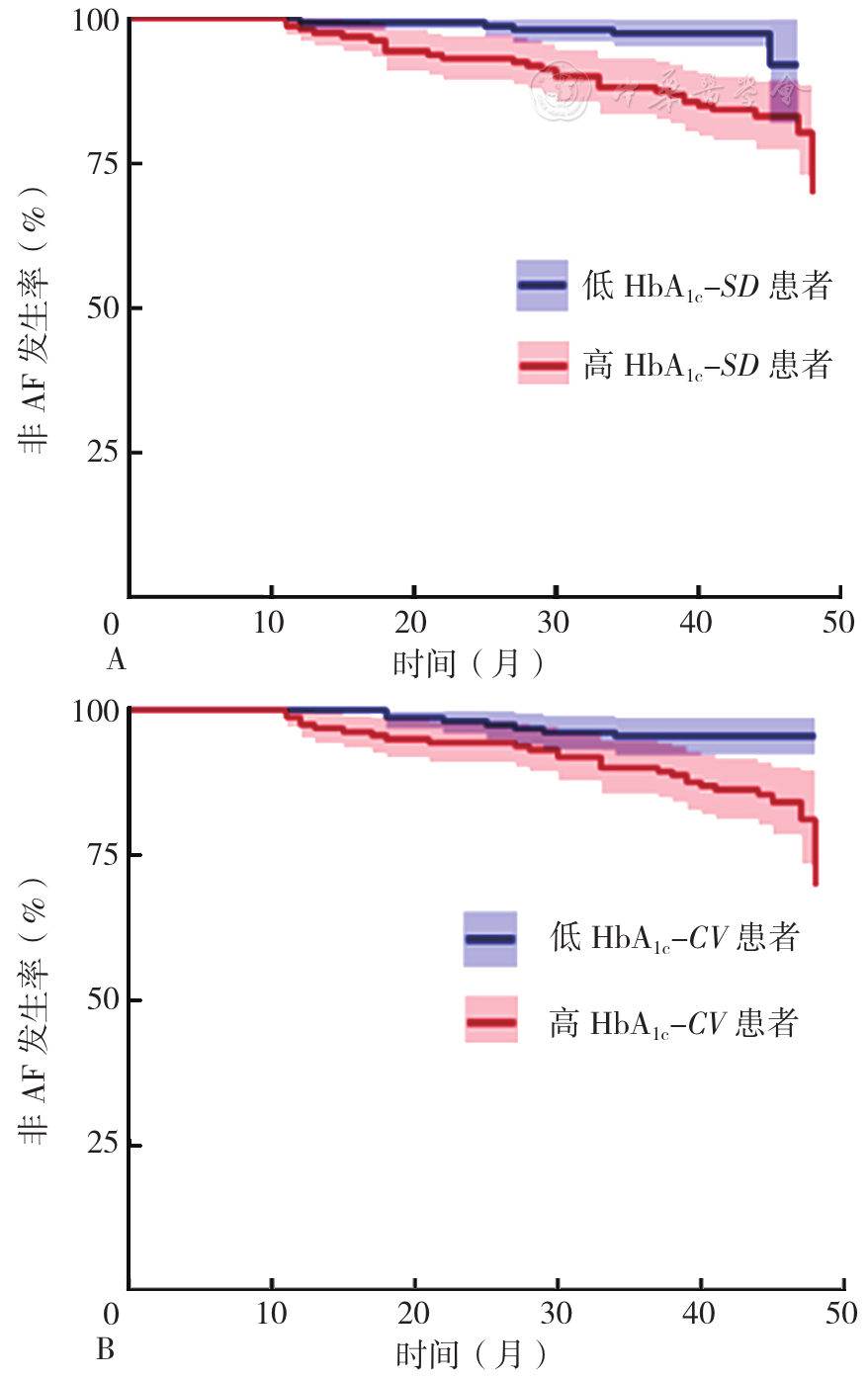
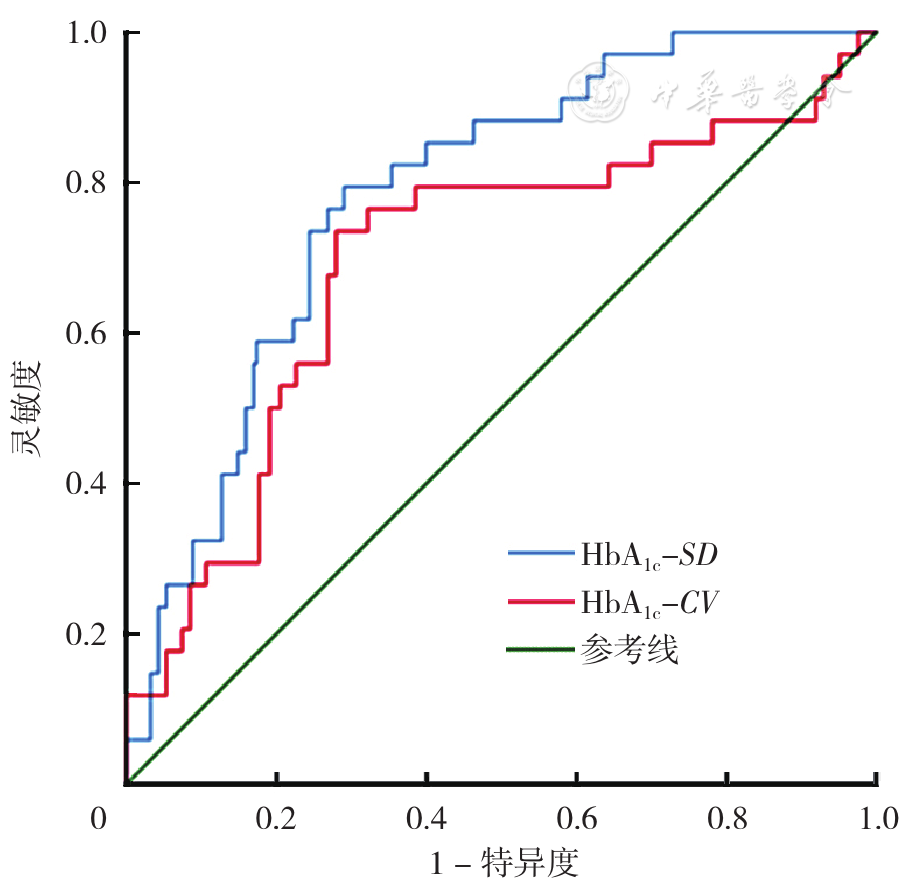
摘要: 背景 糖尿病作为心血管疾病常见的危险因素一直备受关注。糖化血红蛋白(HbA1c)变异性是反映长期血糖波动的指标。因此探讨HbA1c变异性与糖尿病合并射血分数保留心力衰竭(HFpEF)新发心房颤动(AF)的关系具有重要临床意义。 目的 探究在2型糖尿病(T2DM)合并HFpEF患者中,HbA1c变异性与其新发AF的关系。 方法 回顾性分析2018年1月—2019年1月于郑州大学第二附属医院心血管内科确诊为T2DM合并HFpEF患者317例的临床资料。随访截至2022年2月,平均随访时间3.4年。根据随访期内有无新发AF,将患者分为AF组(34例)与非AF组(283例)。HbA1c变异性以HbA1c测量标准差(HbA1c-SD)和HbA1c变异系数(HbA1c-CV)表示。采用多因素Cox回归分析探究HbA1c变异性与T2DM合并HFpEF患者新发AF的关系。采用K-M法绘制生存曲线。绘制HbA1c变异性预测T2DM合并HFpEF患者新发AF的受试者工作特征曲线(ROC曲线)。 结果 AF组患者HbA1c-SD、HbA1c-CV高于非AF组(P<0.05)。依据HbA1c变异性中位数分为低HbA1c变异性患者(HbA1c-SD≤0.34%,HbA1c-CV≤4.74%)和高HbA1c变异性患者(HbA1c-SD>0.34%,HbA1c-CV>4.74%)。Log-rank检验结果显示,高HbA1c变异性患者新发AF发生率高(PHbA1c-SD<0.001、PHbA1c-CV=0.004)。多因素Cox回归分析结果显示,HbA1c-SD〔HR=2.22,95%CI(1.37,3.61),P=0.001〕、HbA1c-CV〔HR=1.65,95%CI(1.01,2.67),P=0.001〕是T2DM合并HFpEF患者新发AF的独立影响因素。HbA1c-SD预测T2DM合并HFpEF发生AF的ROC曲线下面积(AUC)为0.784〔95%CI(0.713,0.855),P=0.001〕,最佳截断值为0.36%,灵敏度为79.4%,特异度为73.1%。HbA1c-CV预测T2DM合并HFpEF发生AF的AUC为0.694〔95%CI(0.591,0.797),P<0.001〕,最佳截断值为4.97%,灵敏度为73.5%,特异度为72.1%。 结论 高HbA1c变异性(HbA1c-SD>0.34%,HbA1c-CV>4.74%)与T2DM合并HFpEF患者新发AF的风险增加独立相关,并在预测该类患者发生AF中具有较大的临床价值。