中国全科医学 ›› 2023, Vol. 26 ›› Issue (26): 3290-3296.DOI: 10.12114/j.issn.1007-9572.2022.0899
所属专题: 泌尿系统疾病最新文章合辑; 肾脏疾病最新文章合辑; 神经系统疾病最新文章合辑; 脑健康最新研究合辑
王晓雯, 肖统领, 王祎, 杨莹, 夏晓爽, 李新*( )
)
WANG Xiaowen, XIAO Tongling, WANG Yi, YANG Ying, XIA Xiaoshuang, LI Xin*()
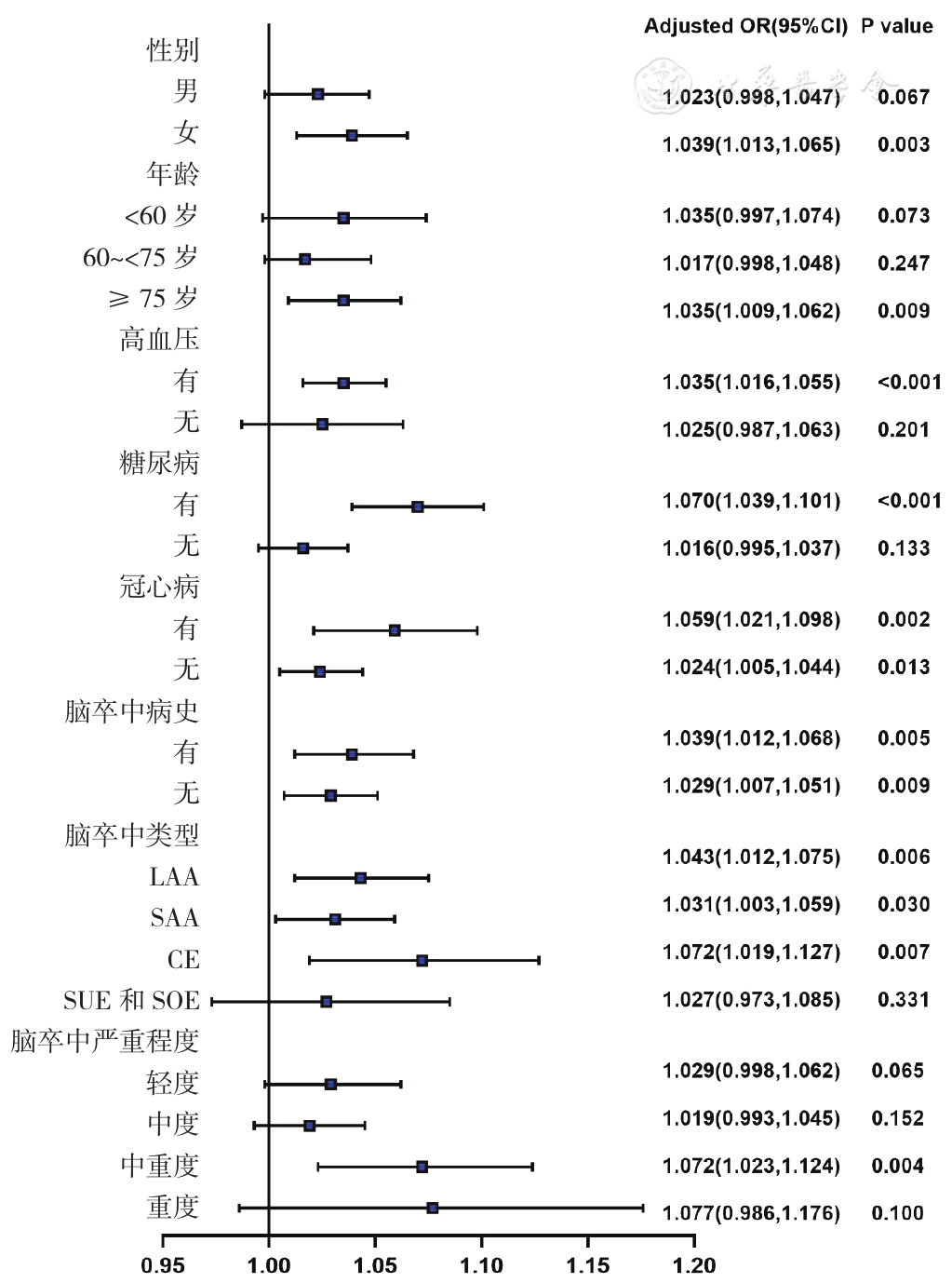
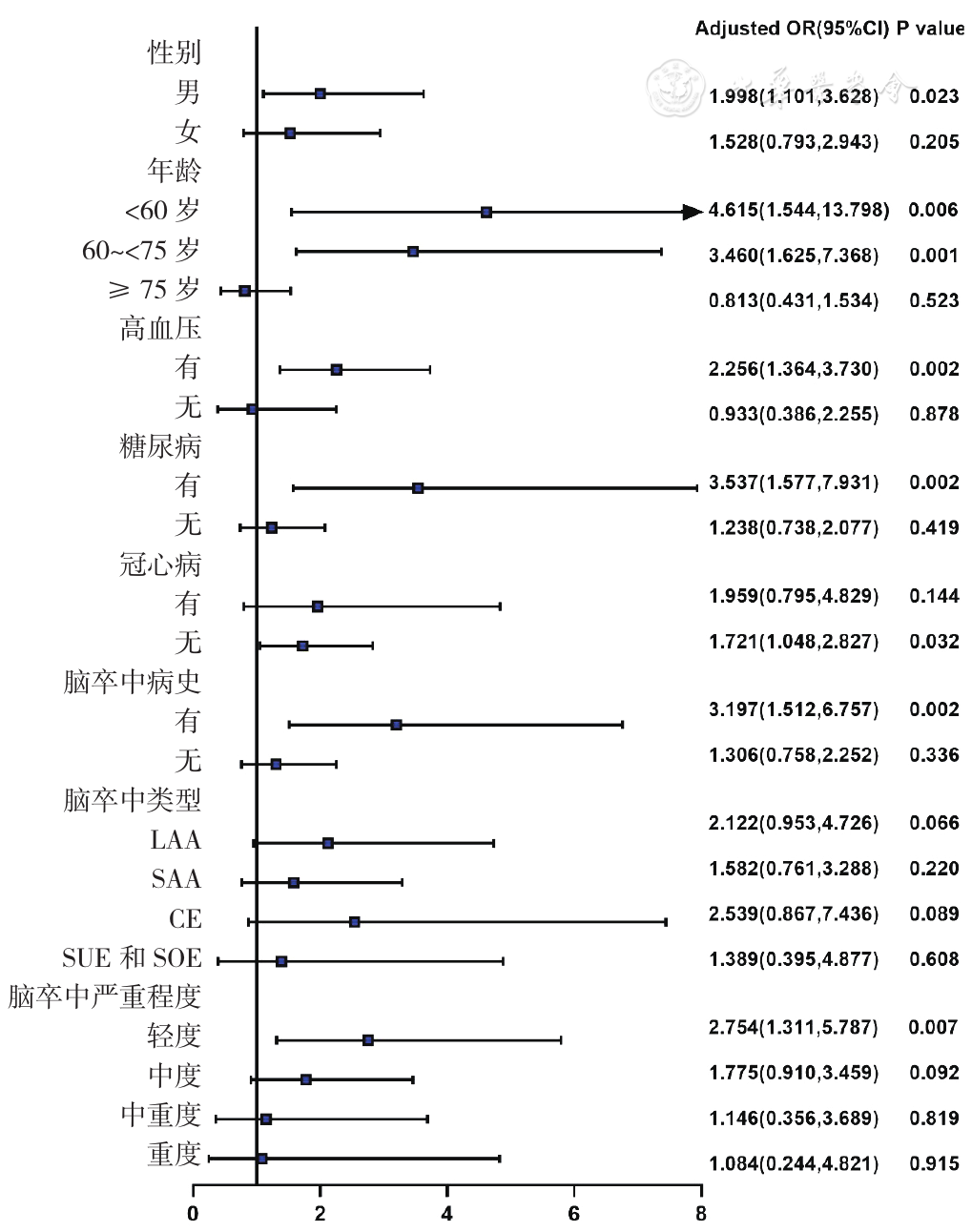
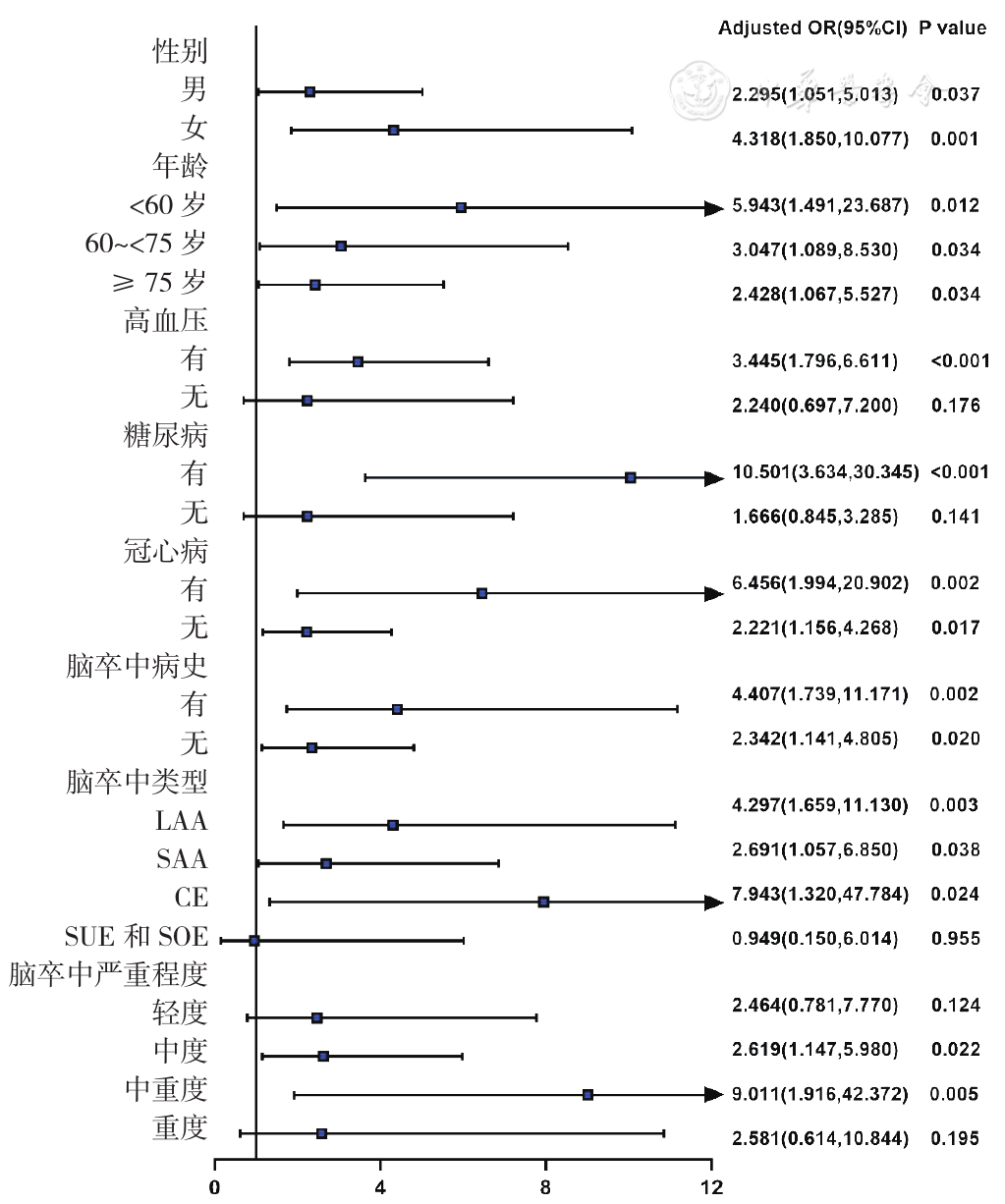
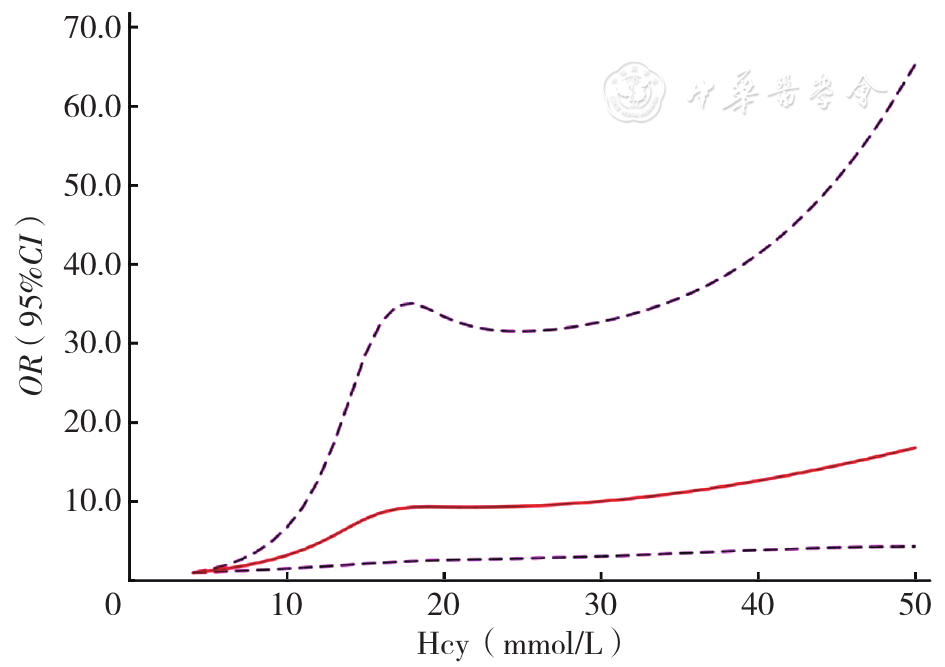
摘要: 背景 急性缺血性脑卒中(AIS)是全球范围内仅次于冠心病的第二大死亡原因,急性肾损伤(AKI)是AIS后较为严重的并发症之一,同型半胱氨酸(Hcy)可能是导致肾损伤和加速肾功能恶化的重要因素。然而目前AIS患者中关于Hcy与AKI关系的研究尚少。 目的 探讨AIS患者Hcy水平与AKI的发生关系,为AIS患者AKI的防治提供更多思路。 方法 纳入2018年1月—2021年4月天津医科大学第二医院神经内科收治的住院AIS患者1 202例为研究对象,通过院内电子病历系统收集基线临床资料。依据《高同型半胱氨酸血症的诊断、治疗与预防专家共识》将患者分为3类:Hcy正常者(Hcy≤15 μmol/L,n=618)、轻型高同型半胱氨酸血症(HHcy)者(Hcy为16~30 μmol/L,n=459)及中重型HHcy者(Hcy>30 μmol/L,n=125)。动态监测患者入院7 d内肾功能和尿量变化,参照2021年改善全球肾脏病预后指南的AKI诊断标准,根据患者是否发生AKI分为AKI组和非AKI组。采用多因素Logistic回归分析探究Hcy分别作为连续变量与分类变量对AIS后发生AKI的影响。采用亚组分析探讨各亚组人群中Hcy与AIS后发生AKI的关系,采用限制性立方样条模型探究Hcy与AIS后发生AKI的非线性关系。 结果 1 202例AIS患者中150例(12.48%)发生AKI(AKI组)。多因素Logistic回归分析结果显示,调整混杂变量后Hcy每升高1 μmol/L,AIS后发生AKI的风险增加〔OR=1.035,95%CI(1.019,1.052),P<0.05〕;以Hcy正常者为参照组,轻型和中重型HHcy者发生AKI的风险均增加〔OR=1.770,95%CI(1.150,2.724),P<0.05;OR=2.927,95%CI(1.671,5.126),P<0.05〕。亚组分析结果显示,Hcy作为连续变量时,在女性、年龄≥75岁、有高血压、有糖尿病、有无脑卒中病史、入院时为中重度脑卒中及脑卒中类型为大动脉粥样硬化型(LAA)、小动脉闭塞型(SAA)或心源性栓塞型(CE)的AIS患者中,AKI的发生风险随Hcy水平的升高而增加(P<0.05)。Hcy作为分类变量时,在男性、<75岁、有高血压、有糖尿病、有脑卒中病史、无冠心病及入院时为轻度脑卒中的AIS患者中,轻型HHcy者较Hcy正常者发生AKI的风险升高(P<0.05)。在女性、有高血压、有糖尿病、无论年龄大小、是否有冠心病、是否有脑卒中病史、入院时为中度或中重度脑卒中及脑卒中类型为LAA、SAA或CE的AIS患者中,中重型HHcy者较Hcy正常者发生AKI的风险升高(P<0.05)。限制性立方样条模型结果显示,Hcy与AKI发生风险之间存在非线性关联,且呈上凸型曲线(P=0.026)。当入院时Hcy<17 mmol/L时,AIS后发生AKI的风险随Hcy的升高快速升高;当入院时Hcy≥17 mmol/L时,AIS后发生AKI的风险随Hcy的升高而缓慢上升。 结论 Hcy无论作为连续变量还是分类变量均是影响AIS后发生AKI的危险因素,监测患者Hcy水平有助于早期识别并预防AKI,改善患者预后。