
中国全科医学 ›› 2023, Vol. 26 ›› Issue (08): 917-926.DOI: 10.12114/j.issn.1007-9572.2022.0592
所属专题: 心血管最新文章合辑
阮海燕1,2, 李丽英1, 张木馨1,3, 郑翼1, 何森1,*( )
)
收稿日期:2022-04-12
修回日期:2022-10-10
出版日期:2023-03-15
发布日期:2022-11-24
通讯作者:
何森
基金资助:
RUAN Haiyan1,2, LI Liying1, ZHANG Muxin1,3, ZHENG Yi1, HE Sen1,*()
Received:2022-04-12
Revised:2022-10-10
Published:2023-03-15
Online:2022-11-24
Contact:
HE Sen
摘要: 背景 血栓栓塞(TE)事件是肥厚型心肌病(HCM)的重要并发症。目前针对HCM患者TE事件的风险预测,仅国外学者构建了两个模型:HCM Risk-CVA及French HCM score,然而,现有研究发现HCM Risk-CVA模型对于中国HCM患者的临床价值较为有限。 目的 本研究拟构建适合中国HCM患者的TE事件风险预测模型。 方法 本研究系回顾性队列研究,收集2010—2018年在四川大学华西医院就诊的537例HCM患者的病例资料。本研究通过电话随访或电子病历系统查询患者就诊记录,每6~12个月随访1次,直至出现终点事件或死亡或研究拟定的评估日期(2019-12-31),终点事件定义为复合性TE事件。采用单因素和多因素Cox回归分析构建风险预测模型,并使用自助重抽样的方法进行内部验证。 结果 537例患者中,24例患者有不同程度的数据缺失,最终纳入513例患者。中位随访时间为4.2(1.3,6.2)年,随访过程中42例(8.18%)发生TE事件,年发病率为2.10%〔95%CI(1.47%,2.73%)〕。根据多因素Cox回归模型构建TE事件风险预测模型,最终纳入年龄、既往TE事件、心房颤动及左心室射血分数(LVEF)(P<0.05)。根据回归系数进行权重后,分别赋值构建SAAE score评分模型,即:S=既往脑卒中(stroke)等TE事件,A=心房颤动(atrial fibrillation),A=年龄(age),E=左心室射血分数(left ventricular ejection fraction)。内部验证提示SAAE score在整体人群中区分TE事件的Harrell's C-指数为0.773〔95%CI(0.688,0.858)〕,校准斜率为1.006;同时,SAAE score在整体人群中对1、3、5年区分TE事件的Harrell's C-指数分别为0.790、0.799及0.735,校准能力较好。此外,SAAE score在合并/不合并心房颤动的人群中区分TE事件的Harrell's C-指数分别为0.669〔95%CI(0.548,0.791)〕及0.647〔95%CI(0.498,0.795)〕,校准能力也较好;同时,在此两类人群中,该模型对1、3、5年TE事件也具有一定价值的区分及校准能力。对于整体人群、合并/不合并心房颤动人群,根据SAAE score进行高危、中危及低危分层后,均可较好区分TE事件的发生。对于整体人群,SAAE score对于TE的区分优于HCM Risk-CVA模型(P=0.013)。临床决策曲线结果提示在不同预测时间点(1、3、5年),SAAE score的净获益均优于HCM Risk-CVA。 结论 本研究在中国HCM患者中构建了针对TE事件的风险预测模型,即SAAE score,该模型可较好地对HCM患者进行TE事件风险分层。
| 变量 | 定义 | 赋值原则 |
|---|---|---|
| 年龄 | 首次评估时的年龄[ | 连续性变量:岁 |
| 既往TE事件 | 根据CHA2DS2-VASc评分模型中的相关定义,为:缺血性脑卒中、短暂性脑缺血发作或外周动脉栓塞[ | 二分类变量:是/否 |
| 血管疾病 | 根据CHA2DS2-VASc评分模型中的相关定义,为:陈旧心肌梗死、外周动脉疾病或主动脉斑块[ | 二分类变量:是/否 |
| 高血压 | 血压值持续或非同日3次以上超过标准血压,即3次非同日收缩压≥140 mm Hg和/或舒张压≥90 mm Hg者,则诊断高血压;如既往诊断高血压,目前服用药物情况下血压处于参考范围,也诊断为高血压[ | 二分类变量:是/否 |
| 糖尿病 | 空腹血糖水平≥7 mmol/L,或有医生诊断的糖尿病史,或服用降糖药物[ | 二分类变量:是/否 |
| 心房颤动 | 诊断依据:存在心房颤动病史,或常规心电图提示心房颤动,或动态心电图提示心房颤动[ | 二分类变量:是/否 |
| MWT | 超声心动图测定的MWT | 连续性变量:mm |
| LA内径 | 超声心动图测定的LA前后径 | 连续性变量:mm |
| LVOTO | 左心室流出道静息压力阶差≥30 mm Hg[ | 二分类变量:是/否 |
| NYHA心功能分级 | Ⅰ级:有心脏病但体力活动不受限制;日常体力活动不引起明显的疲乏、心悸、呼吸困难、心绞痛等症状 | 二分类变量:Ⅲ/Ⅳ级为是,Ⅰ/Ⅱ级为否 |
| Ⅱ级:体力活动轻度受限;休息时无自觉症状,日常活动可出现较明显的上述症状,休息后很快缓解 | ||
| Ⅲ级:体力活动明显受限;休息时可无症状,轻于日常活动即引起上述症状,休息较长时间后方可缓解 | ||
| Ⅳ级:不能从事任何体力活动;休息时亦有心衰的症状,体力活动后明显加重 | ||
| LVEF | 超声心动图测定的左心室射血分数 | 连续性变量:% |
表1 基线评估的候选预测变量定义及赋值原则
Table 1 Definitions and weight assignment principles of candidate variables
| 变量 | 定义 | 赋值原则 |
|---|---|---|
| 年龄 | 首次评估时的年龄[ | 连续性变量:岁 |
| 既往TE事件 | 根据CHA2DS2-VASc评分模型中的相关定义,为:缺血性脑卒中、短暂性脑缺血发作或外周动脉栓塞[ | 二分类变量:是/否 |
| 血管疾病 | 根据CHA2DS2-VASc评分模型中的相关定义,为:陈旧心肌梗死、外周动脉疾病或主动脉斑块[ | 二分类变量:是/否 |
| 高血压 | 血压值持续或非同日3次以上超过标准血压,即3次非同日收缩压≥140 mm Hg和/或舒张压≥90 mm Hg者,则诊断高血压;如既往诊断高血压,目前服用药物情况下血压处于参考范围,也诊断为高血压[ | 二分类变量:是/否 |
| 糖尿病 | 空腹血糖水平≥7 mmol/L,或有医生诊断的糖尿病史,或服用降糖药物[ | 二分类变量:是/否 |
| 心房颤动 | 诊断依据:存在心房颤动病史,或常规心电图提示心房颤动,或动态心电图提示心房颤动[ | 二分类变量:是/否 |
| MWT | 超声心动图测定的MWT | 连续性变量:mm |
| LA内径 | 超声心动图测定的LA前后径 | 连续性变量:mm |
| LVOTO | 左心室流出道静息压力阶差≥30 mm Hg[ | 二分类变量:是/否 |
| NYHA心功能分级 | Ⅰ级:有心脏病但体力活动不受限制;日常体力活动不引起明显的疲乏、心悸、呼吸困难、心绞痛等症状 | 二分类变量:Ⅲ/Ⅳ级为是,Ⅰ/Ⅱ级为否 |
| Ⅱ级:体力活动轻度受限;休息时无自觉症状,日常活动可出现较明显的上述症状,休息后很快缓解 | ||
| Ⅲ级:体力活动明显受限;休息时可无症状,轻于日常活动即引起上述症状,休息较长时间后方可缓解 | ||
| Ⅳ级:不能从事任何体力活动;休息时亦有心衰的症状,体力活动后明显加重 | ||
| LVEF | 超声心动图测定的左心室射血分数 | 连续性变量:% |
| 变量 | 未发生TE事件(n=471) | 发生TE事件(n=42) | χ2(Z)值 | P值 |
|---|---|---|---|---|
| 性别(男/女) | 267/204 | 16/26 | 4.664 | 0.031 |
| 年龄〔M(P25,P75),岁〕 | 57.0(44.0,66.0) | 66.0(51.3,73.0) | 12.027a | 0.001 |
| 既往TE事件〔n(%)〕 | 20(4.25) | 7(16.67) | — | 0.004 |
| 血管疾病〔n(%)〕 | 35(7.43) | 5(11.90) | — | 0.360 |
| 高血压〔n(%)〕 | 147(31.21) | 15(35.71) | 0.184 | 0.668 |
| 糖尿病〔n(%)〕 | 33(7.01) | 7(16.67) | — | 0.035 |
| 心房颤动〔n(%)〕 | 65(13.80) | 22(52.38) | 38.063 | <0.001 |
| MWT〔M(P25,P75),mm〕 | 19.0(17.0,22.0) | 18.0(16.0,21.0) | 2.466a | 0.116 |
| LA内径〔M(P25,P75),mm〕 | 40.0(35.0,45.0) | 43.0(38.2,46.0) | 6.955a | 0.008 |
| LVOTO〔n(%)〕 | 208(44.16) | 14(33.33) | 1.427 | 0.232 |
| NYHA心功能Ⅲ/Ⅳ级〔n(%)〕 | 163(34.61) | 13(30.95) | 0.095 | 0.758 |
| LVEF〔M(P25,P75),%〕 | 69.0(63.0,73.0) | 67.5(62.2,70.0) | 3.712a | 0.054 |
| 阿司匹林〔n(%)〕 | 84(17.83) | 10(23.81) | 0.564 | 0.453 |
| 氯吡格雷〔n(%)〕 | 28(5.94) | 3(7.14) | — | 0.733 |
| 华法林〔n(%)〕 | 35(7.43) | 10(23.81) | — | 0.002 |
表2 未发生TE事件者和发生TE事件者基线特征比较
Table 2 Baseline characteristics in hypertrophic cardiomyopathy patients with and without thrombotic events
| 变量 | 未发生TE事件(n=471) | 发生TE事件(n=42) | χ2(Z)值 | P值 |
|---|---|---|---|---|
| 性别(男/女) | 267/204 | 16/26 | 4.664 | 0.031 |
| 年龄〔M(P25,P75),岁〕 | 57.0(44.0,66.0) | 66.0(51.3,73.0) | 12.027a | 0.001 |
| 既往TE事件〔n(%)〕 | 20(4.25) | 7(16.67) | — | 0.004 |
| 血管疾病〔n(%)〕 | 35(7.43) | 5(11.90) | — | 0.360 |
| 高血压〔n(%)〕 | 147(31.21) | 15(35.71) | 0.184 | 0.668 |
| 糖尿病〔n(%)〕 | 33(7.01) | 7(16.67) | — | 0.035 |
| 心房颤动〔n(%)〕 | 65(13.80) | 22(52.38) | 38.063 | <0.001 |
| MWT〔M(P25,P75),mm〕 | 19.0(17.0,22.0) | 18.0(16.0,21.0) | 2.466a | 0.116 |
| LA内径〔M(P25,P75),mm〕 | 40.0(35.0,45.0) | 43.0(38.2,46.0) | 6.955a | 0.008 |
| LVOTO〔n(%)〕 | 208(44.16) | 14(33.33) | 1.427 | 0.232 |
| NYHA心功能Ⅲ/Ⅳ级〔n(%)〕 | 163(34.61) | 13(30.95) | 0.095 | 0.758 |
| LVEF〔M(P25,P75),%〕 | 69.0(63.0,73.0) | 67.5(62.2,70.0) | 3.712a | 0.054 |
| 阿司匹林〔n(%)〕 | 84(17.83) | 10(23.81) | 0.564 | 0.453 |
| 氯吡格雷〔n(%)〕 | 28(5.94) | 3(7.14) | — | 0.733 |
| 华法林〔n(%)〕 | 35(7.43) | 10(23.81) | — | 0.002 |
| 变量 | 单因素Cox回归分析 | 多因素Cox回归分析 | ||||
|---|---|---|---|---|---|---|
| HR(95%CI) | P值 | β | HR(95%CI) | P值 | ||
| 性别(以男性为参照) | ||||||
| 女 | 1.85(0.99,3.45) | 0.053 | — | — | — | |
| 年龄(岁,以<50岁为参照) | ||||||
| 50~<70 | 1.69(0.73,3.92) | 0.221 | 0.329 | 1.39(0.59,3.28) | 0.452 | |
| ≥70 | 4.46(1.92,10.4) | <0.001 | 1.107 | 3.02(1.25,7.34) | 0.014 | |
| 既往TE事件 | 5.62(2.49,12.7) | <0.001 | 1.174 | 3.24(1.38,7.61) | 0.007 | |
| 血管疾病1 | .92(0.75,4.90) | 0.174 | — | — | — | |
| 高血压 | 1.30(0.69,2.44) | 0.420 | — | — | — | |
| 糖尿病 | 2.20(0.97,4.94) | 0.058 | — | — | — | |
| 心房颤动 | 5.95(3.24,10.90) | <0.001 | 1.472 | 4.36(2.31,8.23) | <0.001 | |
| MWT(mm,以<20.0 mm为参照) | ||||||
| 20.0~<25.0 | 0.98(0.51,1.88) | 0.949 | — | — | — | |
| 25.0~<30.0 | 0.49(0.12,2.09) | 0.338 | — | — | — | |
| ≥30.0 | 0(0,Inf) | 0.996 | — | — | — | |
| LA内径(mm,以<35.0 mm为参照) | ||||||
| 35.0~<40.0 | 1.52(0.47,4.95) | 0.484 | — | — | — | |
| 40.0~<45.0 | 3.14(1.03,9.55) | 0.044 | — | — | — | |
| ≥45.0 | 2.80(0.93,8.44) | 0.067 | — | — | — | |
| LVOTO | 0.72(0.38,1.37) | 0.314 | — | — | — | |
| NYHA心功能分级(以Ⅰ/Ⅱ级为参照) | ||||||
| Ⅲ/Ⅳ级 | 1.05(0.54,2.02) | 0.887 | — | — | — | |
| LVEF(%,以<50.0%为参照) | ||||||
| 50.0~<70.0 | 0.56(0.17,1.86) | 0.344 | -0.981 | 0.37(0.11,1.29) | 0.120 | |
| ≥70.0 | 0.31(0.09,1.08) | 0.067 | -1.407 | 0.24(0.07,0.91) | 0.035 | |
| 阿司匹林 | 1.35(0.67,2.76) | 0.402 | — | — | — | |
| 氯吡格雷 | 1.26(0.39,4.07) | 0.702 | — | — | — | |
| 华法林 | 4.33(2.11,8.89) | <0.001 | — | — | — | |
表3 HCM患者发生TE事件预测的单因素和多因素Cox回归分析
Table 3 Univariate and multvariate Cox regression analyses for factors predicting the risk of thrombotic events in hypertrophic cardiomyopathy patients
| 变量 | 单因素Cox回归分析 | 多因素Cox回归分析 | ||||
|---|---|---|---|---|---|---|
| HR(95%CI) | P值 | β | HR(95%CI) | P值 | ||
| 性别(以男性为参照) | ||||||
| 女 | 1.85(0.99,3.45) | 0.053 | — | — | — | |
| 年龄(岁,以<50岁为参照) | ||||||
| 50~<70 | 1.69(0.73,3.92) | 0.221 | 0.329 | 1.39(0.59,3.28) | 0.452 | |
| ≥70 | 4.46(1.92,10.4) | <0.001 | 1.107 | 3.02(1.25,7.34) | 0.014 | |
| 既往TE事件 | 5.62(2.49,12.7) | <0.001 | 1.174 | 3.24(1.38,7.61) | 0.007 | |
| 血管疾病1 | .92(0.75,4.90) | 0.174 | — | — | — | |
| 高血压 | 1.30(0.69,2.44) | 0.420 | — | — | — | |
| 糖尿病 | 2.20(0.97,4.94) | 0.058 | — | — | — | |
| 心房颤动 | 5.95(3.24,10.90) | <0.001 | 1.472 | 4.36(2.31,8.23) | <0.001 | |
| MWT(mm,以<20.0 mm为参照) | ||||||
| 20.0~<25.0 | 0.98(0.51,1.88) | 0.949 | — | — | — | |
| 25.0~<30.0 | 0.49(0.12,2.09) | 0.338 | — | — | — | |
| ≥30.0 | 0(0,Inf) | 0.996 | — | — | — | |
| LA内径(mm,以<35.0 mm为参照) | ||||||
| 35.0~<40.0 | 1.52(0.47,4.95) | 0.484 | — | — | — | |
| 40.0~<45.0 | 3.14(1.03,9.55) | 0.044 | — | — | — | |
| ≥45.0 | 2.80(0.93,8.44) | 0.067 | — | — | — | |
| LVOTO | 0.72(0.38,1.37) | 0.314 | — | — | — | |
| NYHA心功能分级(以Ⅰ/Ⅱ级为参照) | ||||||
| Ⅲ/Ⅳ级 | 1.05(0.54,2.02) | 0.887 | — | — | — | |
| LVEF(%,以<50.0%为参照) | ||||||
| 50.0~<70.0 | 0.56(0.17,1.86) | 0.344 | -0.981 | 0.37(0.11,1.29) | 0.120 | |
| ≥70.0 | 0.31(0.09,1.08) | 0.067 | -1.407 | 0.24(0.07,0.91) | 0.035 | |
| 阿司匹林 | 1.35(0.67,2.76) | 0.402 | — | — | — | |
| 氯吡格雷 | 1.26(0.39,4.07) | 0.702 | — | — | — | |
| 华法林 | 4.33(2.11,8.89) | <0.001 | — | — | — | |
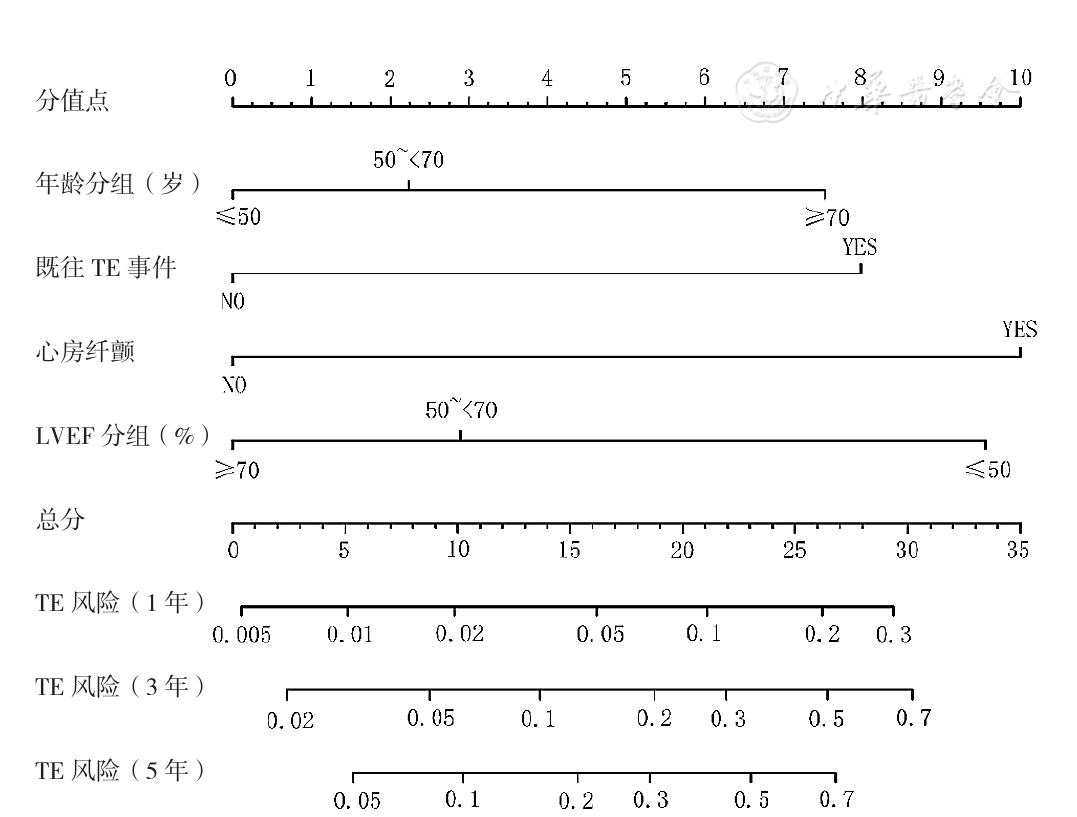
图1 HCM患者发生TE事件风险预测的诺曼图注:LVEF=左心室射血分数,TE=血栓栓塞
Figure 1 Nomangram for risk prediction of thrombotic events in hypertrophic cardiomyopathy patients
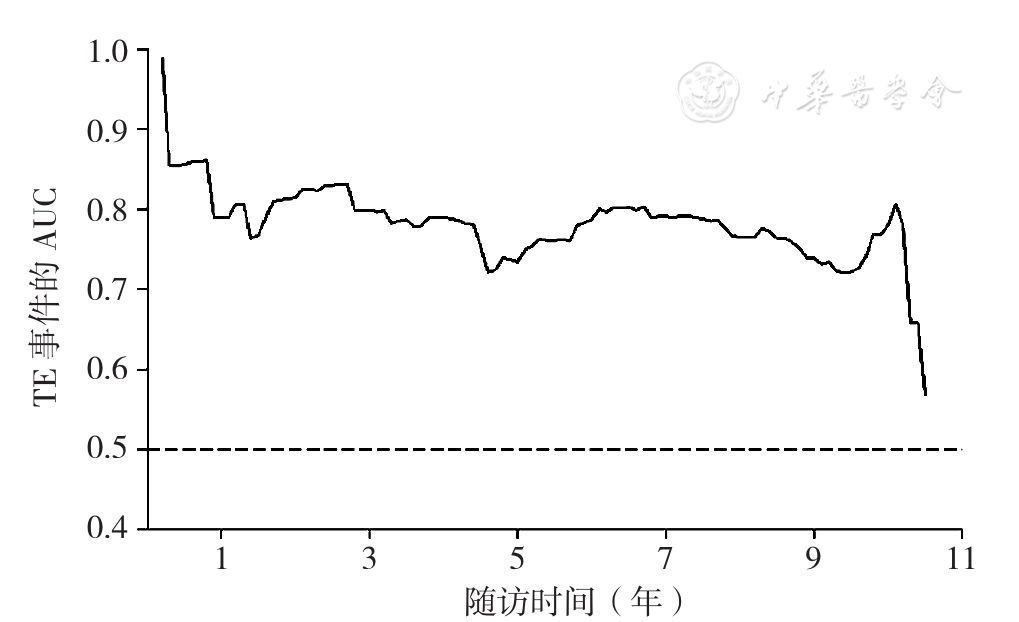
图2 SAAE score对整体人群1、3、5年TE事件的区分能力注:AUC=曲线下面积
Figure 2 Predictive power of SAAE score for 1-,3- and 5-year risk of thrombotic events in the whole study population
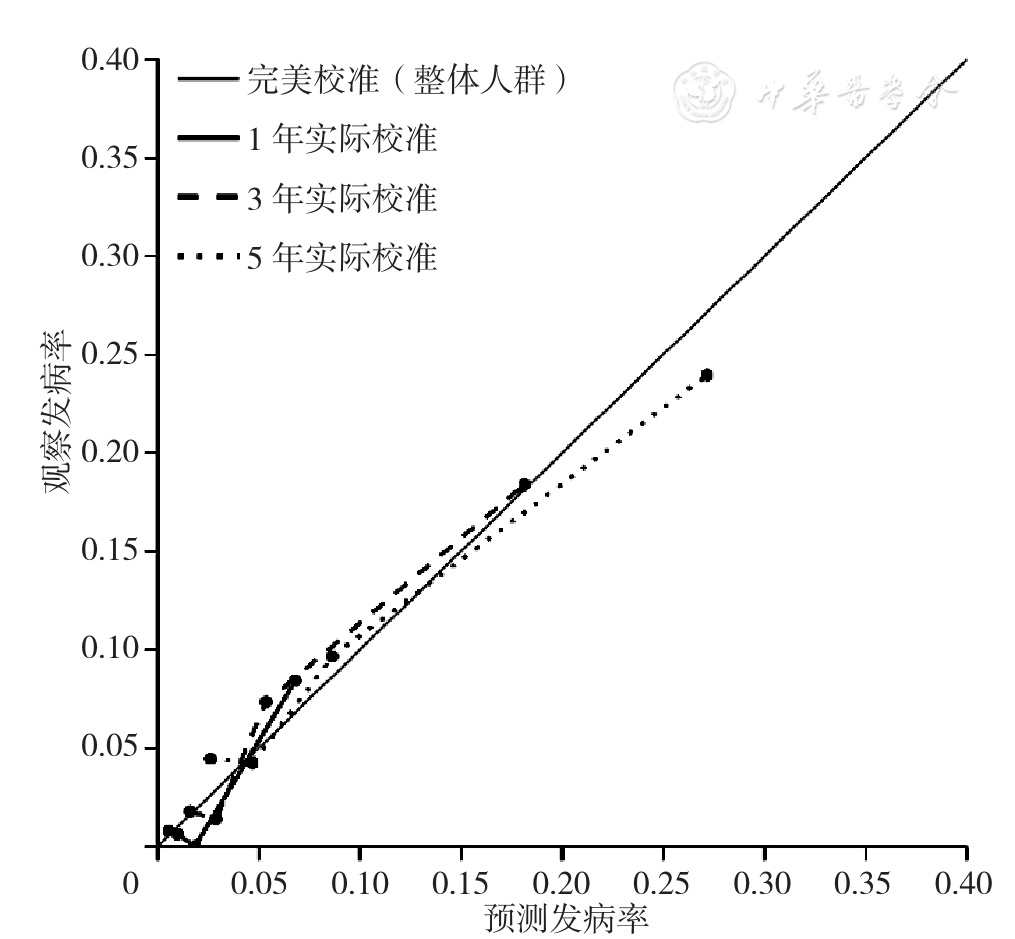
图3 SAAE score对整体人群1、3、5年TE事件的校准能力
Figure 3 Calibration plots for predicted versus observed 1-,3-,5-year risk of thrombotic events for whole study population
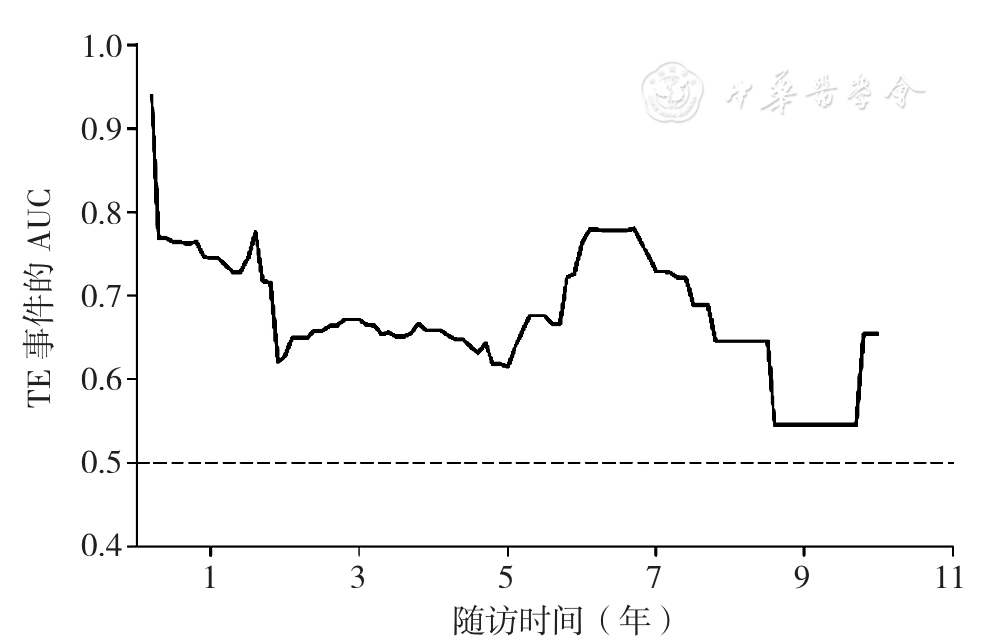
图4 SAAE score对心房颤动人群1、3年及5年TE事件的区分能力
Figure 4 Predictive power of SAAE score for 1-,3-,5-year risk of thrombotic events for hypertrophic cardiomyopathy patients with atrial fibrillation
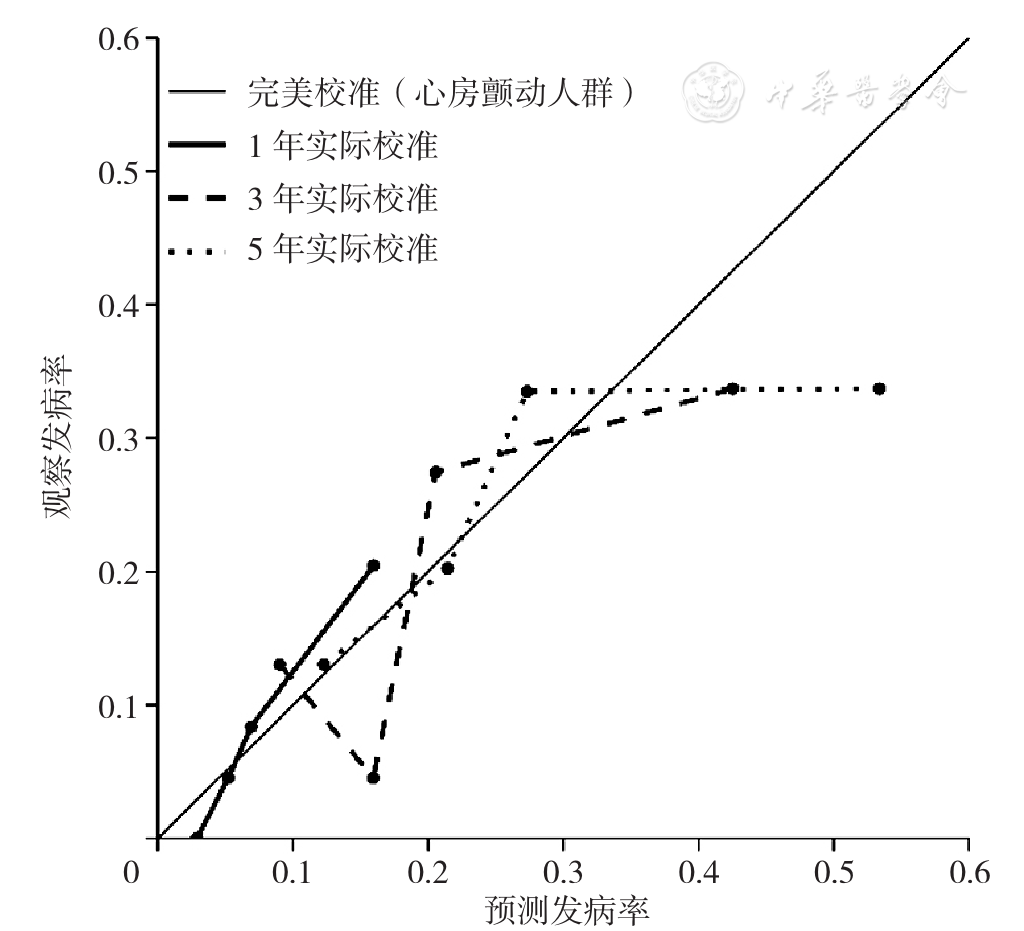
图5 SAAE score对心房颤动人群1、3、5年TE事件的校准能力
Figure 5 Calibration plots for predicted versus observed 1-,3-,5-year risk of thrombotic events for hypertrophic cardiomyopathy patients with atrial fibrillation
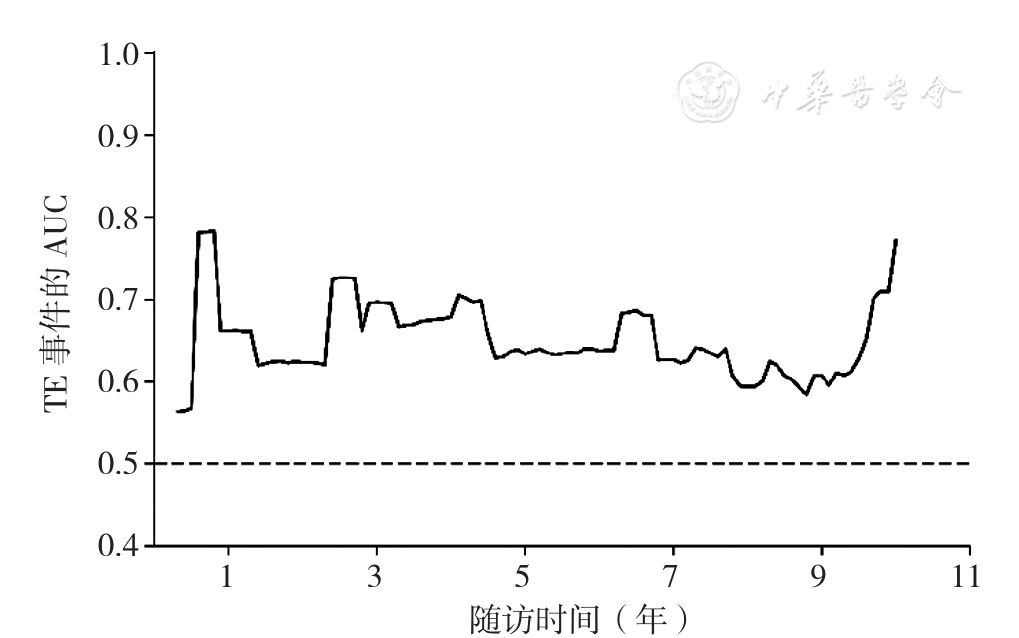
图6 SAAE score对非心房颤动人群1、3、5年TE事件的区分能力
Figure 6 Predictive power of SAAE score for 1-,3- and 5-year risk of thrombotic events for hypertrophic cardiomyopathy patients without atrial fibrillation
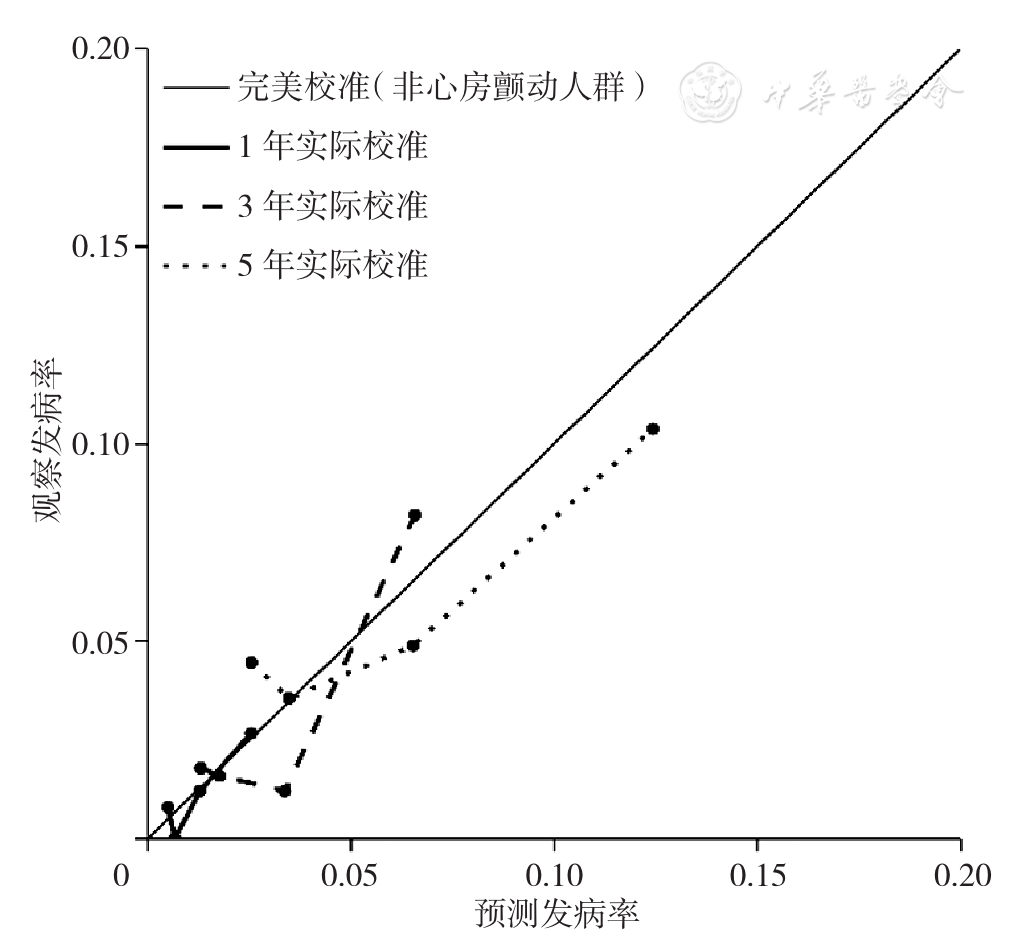
图7 SAAE score对非心房颤动人群1、3年及5年TE事件的校准能力
Figure 7 Calibration plots for predicted versus observed 1-,3-,5-year risk of thrombotic events for hypertrophic cardiomyopathy patients without atrial fibrillation
| 分类 | 低风险 | 中风险 | 高风险 |
|---|---|---|---|
| 整体人群 | <7.56 | 7.56~<17.38 | ≥17.38 |
| 心房颤动人群 | <17.56 | 17.56~<21.42 | ≥21.42 |
| 非心房颤动人群 | <3.87 | 3.87~<11.25 | ≥11.25 |
表4 SAAE score预测整体人群、心房颤动人群和非心房颤动人群发生TE事件的低、中、高风险分值(分)
Table 4 Cutoff points of SAAE score for low,moderate and high risk of thrombotic events in different populations
| 分类 | 低风险 | 中风险 | 高风险 |
|---|---|---|---|
| 整体人群 | <7.56 | 7.56~<17.38 | ≥17.38 |
| 心房颤动人群 | <17.56 | 17.56~<21.42 | ≥21.42 |
| 非心房颤动人群 | <3.87 | 3.87~<11.25 | ≥11.25 |
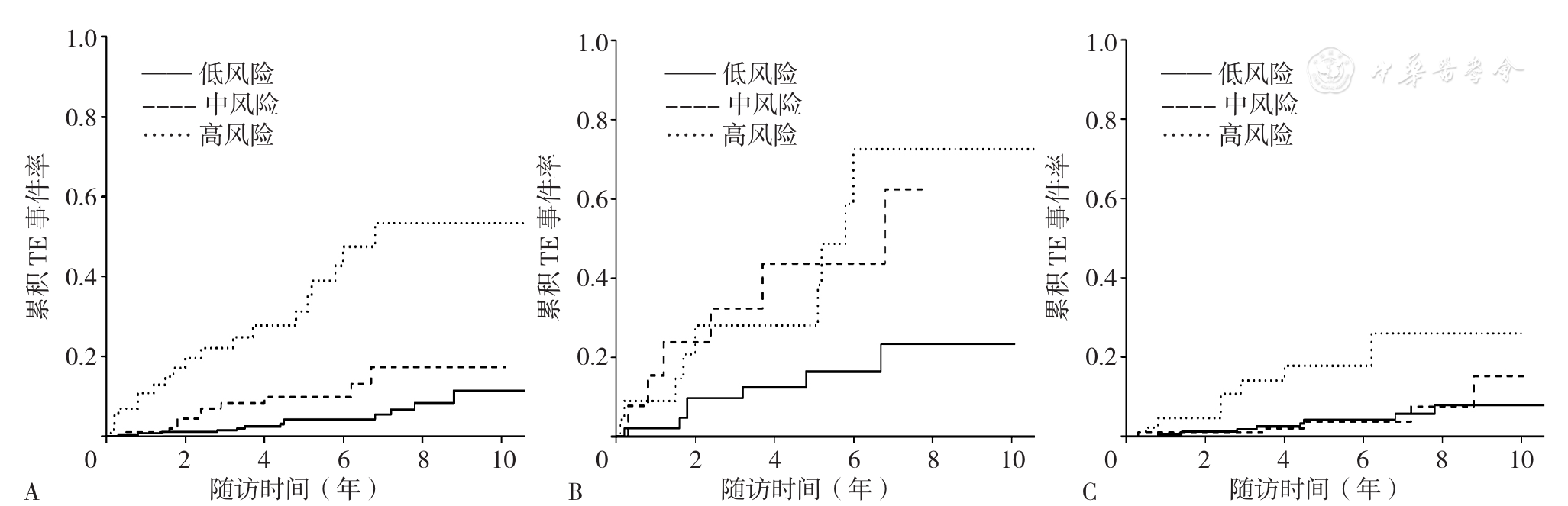
图8 SAAE score对于不同人群危险分组的Kaplan-Meier曲线分析注:A为整体人群,B为心房颤动人群,C为非心房颤动人群
Figure 8 Kaplan-Meier analysis showing cumulative thrombotic events in hypertrophic cardiomyopathy patients with low,moderate or high thrombotic risk predicted by SAAE score
| 人群 | 评分模型 | 整体 | 1年 | 3年 | 5年 | ||||
|---|---|---|---|---|---|---|---|---|---|
| Harrell's C-指数 | P值 | Harrell's C-指数 | P值 | Harrell's C-指数 | P值 | Harrell's C-指数 | P值 | ||
| 整体人群 | SAAE score | 0.757 | 0.013 | 0.790 | 0.413 | 0.799 | 0.137 | 0.735 | 0.117 |
| HCM Risk-CVA | 0.671 | 0.710 | 0.715 | 0.670 | |||||
| 心房颤动人群 | SAAE score | 0.670 | 0.110 | 0.745 | 0.112 | 0.671 | 0.162 | 0.616 | 0.738 |
| HCM Risk-CVA | 0.560 | 0.557 | 0.538 | 0.587 | |||||
| 非心房颤动人群 | SAAE score | 0.624 | 0.549 | 0.661 | 0.828 | 0.697 | 0.899 | 0.634 | 0.644 |
| HCM Risk-CVA | 0.592 | 0.696 | 0.710 | 0.603 | |||||
表5 SAAE score与HCM Risk-CVA模型区分TE事件的对比
Table 5 Comparisons between SAAE score and HCM Risk-CVA score for predicting the risk of thrombotic events in hypertrophic cardiomyopathy
| 人群 | 评分模型 | 整体 | 1年 | 3年 | 5年 | ||||
|---|---|---|---|---|---|---|---|---|---|
| Harrell's C-指数 | P值 | Harrell's C-指数 | P值 | Harrell's C-指数 | P值 | Harrell's C-指数 | P值 | ||
| 整体人群 | SAAE score | 0.757 | 0.013 | 0.790 | 0.413 | 0.799 | 0.137 | 0.735 | 0.117 |
| HCM Risk-CVA | 0.671 | 0.710 | 0.715 | 0.670 | |||||
| 心房颤动人群 | SAAE score | 0.670 | 0.110 | 0.745 | 0.112 | 0.671 | 0.162 | 0.616 | 0.738 |
| HCM Risk-CVA | 0.560 | 0.557 | 0.538 | 0.587 | |||||
| 非心房颤动人群 | SAAE score | 0.624 | 0.549 | 0.661 | 0.828 | 0.697 | 0.899 | 0.634 | 0.644 |
| HCM Risk-CVA | 0.592 | 0.696 | 0.710 | 0.603 | |||||
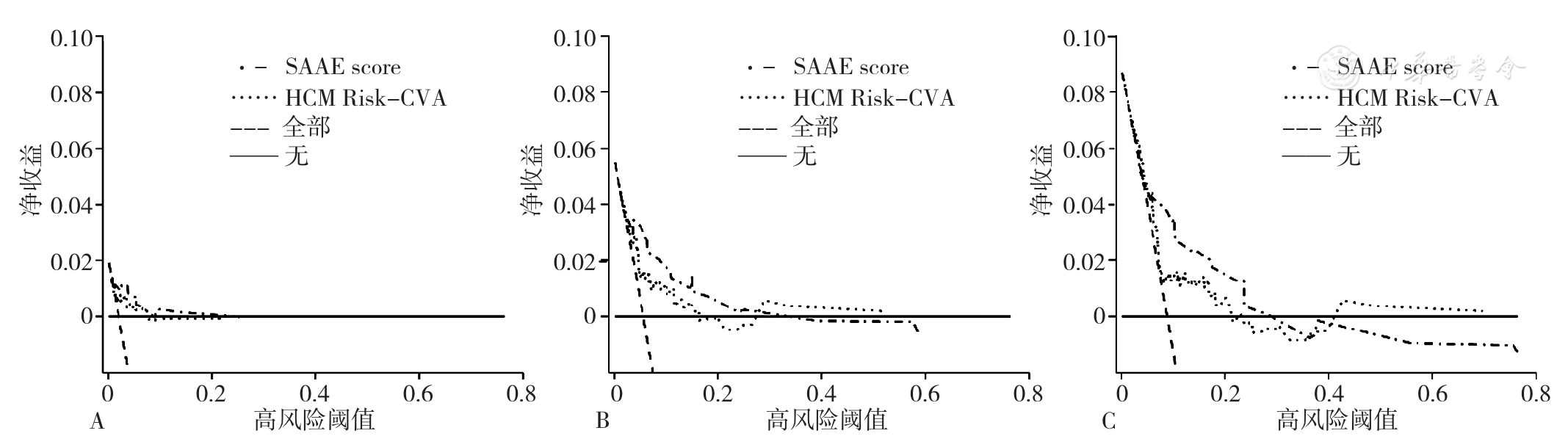
图9 SAAE score及HCM Risk-CVA在不同预测时间点的临床决策曲线注:A为1年,B为3年,C为5年
Figure 9 Decision curve analysis of SAAE score and HCM Risk-CVA score for predicting the risk of thrombotic events in hypertrophic cardiomyopathy at different time points
| [1] |
|
| [2] |
|
| [3] |
吴兆苏,姚崇华,赵冬. 我国人群脑卒中发病率、死亡率的流行病学研究[J]. 中华流行病学杂志,2003,24(3):236-239.
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
《中国高血压防治指南》修订委员会. 中国高血压防治指南2018年修订版[J]. 心脑血管病防治,2019,19(1):1-44. DOI:10.3969/j.issn.1009-816X.2019.01.001.
|
| [21] |
American Diabetes Association. Standards of medical care in diabetes—2010[J]. Diabetes Care,2010,33(Suppl 1):S11-61. DOI:10.2337/dc10-S011.
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
顾俊,贾锋鹏,封盼攀. CHADS2与CHA2DS2-VASc评分对非瓣膜病房颤患者左房血栓的风险评估[J]. 南方医科大学学报,2014,34(11):1601-1605.
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [1] | 杨晓峰, 李现文, 吴岩峰, 张倩, 陈娟, 赵凤姣. 血管内皮细胞钙黏蛋白水平与急性缺血性脑卒中后认知障碍发生风险的相关性研究[J]. 中国全科医学, 2026, 29(20): 2867-2873. |
| [2] | 李超辉, 刘慧, 王凯. 持续性心房颤动的影响因素识别及判别模型构建研究[J]. 中国全科医学, 2026, 29(20): 2846-2853. |
| [3] | 刘影, 刘世炜, 张驰, 沈姞, 张玉珊, 张洁, 桑莹宸, 王友娇, 王蕾, 周厚广, 施红. 中国老年脑卒中患者主观认知功能下降流行特征及影响因素研究[J]. 中国全科医学, 2026, 29(20): 2829-2835. |
| [4] | 张泽宇, 李春晖. 1990—2021年中国归因于二手烟的缺血性心脏病疾病负担分析[J]. 中国全科医学, 2026, 29(20): 2903-2912. |
| [5] | 吴一璇, 肖亮满, 刘鑫, 严梓萁, 王毓婷, 林舒敏, 庄礼兴. 1990—2021年中国与全球帕金森病的疾病负担分析与未来趋势预测[J]. 中国全科医学, 2026, 29(20): 2895-2902. |
| [6] | 陈歆怡, 黄紫千, 陈昱丰, 黄俊, 翁帆, 赖志胜, 薛玉梅, 曹希. MyDiagnostick手持式单导联心电设备心房颤动检测效能及其在社区人群中的筛查效果研究[J]. 中国全科医学, 2026, 29(19): 2717-2723. |
| [7] | 吴瑞宁, 周明, 张攻孜, 李军, 谢苏杭, 刘杨晓雪, 张佳丽, 刘毛毛, 黄丽萍. 固定式与移动式外骨骼机器人改善脑卒中患者下肢功能及生活质量:一项随机对照试验[J]. 中国全科医学, 2026, 29(17): 2326-2333. |
| [8] | 季颖, 郭川, 朱仕哲, 季盼盼, 王彤, 阚超杰, 王庆雷. 间歇性θ短阵脉冲刺激小脑改善幕上卒中患者多维度平衡功能的疗效:一项随机对照试验[J]. 中国全科医学, 2026, 29(15): 2022-2028. |
| [9] | 李世龙, 王贺, 周晓宇, 付蕾, 赵倬, 华成俊, 司春婴. 心脏巨噬细胞在射血分数保留型心力衰竭中的研究进展[J]. 中国全科医学, 2026, 29(15): 2084-2091. |
| [10] | 韩悦, 边哲, 谷昊辰, 王大力, 彭延波. 他汀类药物累积限定日剂量对缺血性脑卒中复发风险的研究[J]. 中国全科医学, 2026, 29(14): 1821-1826. |
| [11] | 田安妮, 杨晶, 孙晶, 王诗纯. 康复机器人辅助训练对不同阶段脑卒中患者手运动功能恢复效果的Meta分析[J]. 中国全科医学, 2026, 29(14): 1911-1920. |
| [12] | 袁维霞, 敖盼盼, 马芸, 吴风富, 徐发翠, 余娟, 曾群, 魏绍峰, 袁丽佳. 年龄校正的Charlson合并症指数对老年患者肌少症的预测价值研究[J]. 中国全科医学, 2026, 29(13): 1673-1681. |
| [13] | 刘洋, 梁芳, 吴玲, 李文磊, 李鹏飞. 非常规脂质以及甘油三酯-葡萄糖指数诊断初发急性缺血性脑卒中的价值研究[J]. 中国全科医学, 2026, 29(11): 1422-1429. |
| [14] | 张惠娟, 李星辉, 张小明, 尹龙, 邵龙. 选择性心肌肌球蛋白抑制剂治疗肥厚型心肌病有效性和安全性的Meta分析[J]. 中国全科医学, 2026, 29(09): 1194-1202. |
| [15] | 王小楠, 阮晓楠, 刘杨, 吴抗, 邱桦, 刘庆平, 宋家慧, 高娇娇, 周弋, 刘晓琳. 不同身体测量指标与脑卒中发病风险的巢式病例对照研究[J]. 中国全科医学, 2026, 29(08): 1020-1028. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||










